The SCF/KIT Pathway's Roles: Interest in Therapeutic Targets Is Growing
The breadth of the stem cell factor (SCF)/ KIT signaling pathway oncogenic functions and potential role as a therapeutic target are just now becoming clear.


Structure of the KIT protein
The importance of the stem cell factor (SCF)/ KIT signaling pathway in the normal human body is relatively well understood, but the breadth of its oncogenic functions and potential role as a therapeutic target are only just becoming clear.
Agents targeting this pathway have proved more successful in some tumor types than in others; particularly variable has been the role of imatinib (Gleevec, Novartis). More recently, the evolution of a new paradigm of cancer therapy, in which the molecular characteristics of a tumor are used to guide therapeutic regimens for each individual patient, has seemingly brought the story of the SCF/ KIT pathway full circle and is driving increased interest in these agents.
How the Pathway Is Activated
The significant genetic player in this pathway is the KIT gene, whose KIT protein product is a member of the class III receptor tyrosine kinases (RTKs), a family that includes other receptors such as platelet-derived growth factor receptor (PDGFR). As with other RTKs, the binding of a specific ligand, in this case SCF, leads to receptor dimerization (one receptor molecule binding to another), which activates the intrinsic tyrosine kinase activity of the receptor, leading to its phosphorylation at key amino acid residues.
Schematic of KIT Signaling Pathways


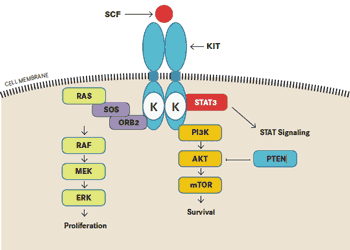
SCF indicates stem cell factor; STAT3, signal transducer and activator of transcription 3; K, tyrosine kinase domain. The MAPK pathway is denoted as RASRAF- MEK-ERK and the PI3K pathway is PI3K-AKT-mTOR.
Adapted from Lovly C, Pao W, Sosman J. KIT in thymic carcinoma: what is KIT? Vanderbilt-Ingram Cancer Center. www.vicc.org. Updated June 30, 2011. Accessed July 25, 2011.
These residues subsequently act as binding sites for signaling molecules within the cell; thus, the process of signal transduction is initiated downstream of the receptor. A number of important downstream signaling cascades are activated by the SCF/KIT pathway including mitogen-activated protein kinase (MAPK) and phosphatidylinositol 3-kinase (PI3K) signaling.
Researchers have identified 2 isoforms of the SCF ligand that are quite different in the signaling outcomes they initiate. The isoforms differ in the presence or absence of a proteolytic cleavage site, and their resulting solubility (let’s call them “SCF ” and “SCF-” for simplicity’s sake). SCF initiates a rapid and transient activation of KIT, followed by a rapid degradation, while SCF- leads to a more sustained activation and prolonged downstream signaling.
The SCF/KIT pathway is believed to have a number of major in vivo functions in humans. Like the JAK/STAT pathway described in last month’s “Pathways” article, SCF/KIT signaling is crucial for hematopoiesis, the formation of blood cells. It plays a particularly vital role in the development of primitive hematopoietic cells such as stem and progenitor cells, becoming less important once they have differentiated, such that less than 0.1% of peripheral blood cells express KIT. One important exception is the mast cells, which continue to express KIT at high levels and are dependent on SCF/KIT signaling for their growth, survival, and proper function.
Another important function of the SCF/KIT pathway is in pigmentation, since it has a very well-established role in melanocyte development. Mice with reduced KIT expression have defective pigmentation, and mutations in the KIT gene have been detected in the majority of humans with piebaldism, a rare inherited condition characterized by a patch of white hair above the forehead.
SCF/KIT signaling is also important in the gastrointestinal tract (specifically in the development of the interstitial cells of Cajal [ICC]), in fertility, and in the nervous system.
Defective SCF/KIT Signaling in Cancer
This myriad of important cellular functions of course translates into a darker side of this pathway, when mutations or altered expression of its component parts lead to the development of cancer.
Unsurprisingly, KIT is associated with several malignant human diseases, which mirror its major in vivo functions, including melanoma, mastocytosis (characterized by an accumulation of mast cells in various tissues), gastrointestinal stromal tumors (GISTs; the most common form of mesenchymal tumor of the digestive tract, thought to arise from the ICC), acute myelogenous lymphoma (AML), and small cell lung carcinoma (SCLC). It also has been described in a range of other tumors such as neuroblastoma, cervical, testicular, thyroid, breast, colon, bladder, renal, pancreatic, and non-small cell lung carcinoma.
However, the precise role of KIT in these different tumors is often complex and poorly understood. While KIT is overexpressed in some melanomas, progression to invasive and metastatic stages has also been shown to correlate with reduced levels of the protein, suggesting a tumor-suppressive function.
In the majority of cases, however, tumors arise from activating mutations in KIT or its overexpression. For example, between 50% and 80% of GISTs have an activating mutation in KIT, and between 28% and 88% of SCLC cell lines have been reported to overexpress KIT. Furthermore, mutations in the kinase domain (D816V) of KIT have been identified in the mast cells of patients with mastocytosis.
New KIT Research Emerging
No KIT-specific inhibitors have been generated to date; however, the tyrosine kinase inhibitor (TKI) imatinib is multitargeted, and also inhibits KIT activity. When it comes to tumors associated with KIT abnormalities, GISTs have been the real success story for imatinib.
Prior to the 2001 approval of the so-called “magic bullet,” patients with GISTs that harbor a KIT mutation had a particularly poor prognosis. Imatinib revolutionized the treatment of these tumors, with more than 80% of patients responding. At the 2011 American Society of Clinical Oncology (ASCO) meeting, the results of an Australian population-based study put the impact of imatinib on GISTs into perspective, showing a 64% improvement in survival of GIST patients subsequent to imatinib approval.
Not all KIT-defective tumors have displayed such dramatic effects, however. Imatinib proved relatively ineffective in the treatment of mastocytosis and controversial in the treatment of melanomas, with several phase II studies reporting no clinical activity in metastatic melanoma. Furthermore, a new problem developed in GIST patients being treated with imatinib: resistance.
For these reasons, researchers began to look for alternative treatments for cases in which imatinib fails to work or when resistance develops. Sunitinib (Sutent, Pfizer) was the first targeted therapy to show effectiveness in treating imatinib-refractory GISTs.
However, a wealth of clinical trial data presented at this year’s ASCO meeting in Chicago highlight the number of second-generation TKIs that are now being tested in this respect, including sorafenib (Nexavar, Bayer Health- Care and Onyx Pharmaceuticals), nilotinib (Tasigna, Novartis), dasatinib (Sprycel, Bristol- Myers Squibb), and regorafenib (BAY 73- 4506, Bayer HealthCare), all TKIs that include KIT among their multiple targets.
The studies presented at ASCO demonstrated that these agents have significant activity in patients with imatinib-resistant GISTs. Some studies also examined patients with sunitinib-resistant GISTs, and these patients also responded well to other second-generation TKIs.
In addition to these alternative agents, the molecular analysis of tumors has now led us full circle back to imatinib, and the case is slowly being made for reassessment of this agent for treatment of melanomas.
Many of the original trials that demonstrated limited clinical activity were carried out prior to the discovery that activating mutations in KIT were important in melanoma development, and therefore did not screen for patients with these mutations. Substantial evidence now suggests that KIT-mutated melanomas can respond to treatment with imatinib.
Melanoma cell lines with KIT mutations are sensitive to imatinib, and numerous studies show that patients with melanoma harboring KIT mutations can have significant and durable clinical responses, with even greater activity in tumors that have certain types of mutations. It is left to the future of SCF/KIT pathway research to determine precisely which KIT alterations may be of particular functional relevance in leading to tumor formation and determining response to treatment.
Jane de Lartigue, PhD, is a freelance medical writer and editor based in the United Kingdom.
Key Research
- Carvajal RD, Antonescu CR, Wolchok JD, et al. KIT as a therapeutic target in metastatic melanoma. JAMA. 2011;305(22):2327-2334.
- George S, von Mehren M, Heinrich C, et al. A multicenter phase II study of regorafenib in patients with advanced gastrointestinal stromal tumor (GIST) after therapy with imatinib and sunitinib. J Clin Oncol. 2011;29(suppl; abstr 10007).
- Goldstein D, Lee C, Tracey E, et al. Validating innovation: A population-based study of gastrointestinal stromal tumors (GIST) to estimate the survival benefit of imatinib. J Clin Oncol. 2011;29(suppl; abstr 10060).
- Guo J, Si L, Kong Y, et al. Phase II, open-label, single-arm trial of imatinib mesylate in patients with metastatic melanoma harboring c-Kit mutation or amplification [Epub ahead of print]. J Clin Oncol. 2011;29(21):2904-2909.
- Kindler HL, Campbell NP, Wroblewski K, et al. Sorafenib in patients with imatinib and sunitinib-resistant gastrointestinal stromal tumors (GIST): final results of a University of Chicago phase II consortium trial. J Clin Oncol. 2011;29(suppl; abstr 10009).
- Lennartsson J, Voytyuk O, Heiss E, et al. C-Kit signal transduction and involvement in cancer. Cancer Ther. 2005;3:5-28.
- Lennartsson J, Rοnnstrand L. The stem cell factor receptor/c-Kit as a drug target in cancer. Curr Cancer Drug Targets. 2006;6(1):561-571.
- Trent JC, Wathen K, von Mehren M, et al. A phase II study of dasatinib for patients with imatinib-resistant gastrointestinal stromal tumor (GIST). J Clin Oncol. 2011;29(suppl; abstr 10006).
















 advances in the next 5 to 10 years.")












