Publication
Article
ASCO Guidelines on VTE Add New Oral Agents
Author(s):
Updated venous thromboembolism (VTE) guidelines issued by the American Society of Clinical Oncology now include the use of direct oral anticoagulants for patients with cancer as a preventive measure against VTE recurrence.


Gary H. Lyman, MD, MPH

Gary H. Lyman, MD, MPH
Updated venous thromboembolism (VTE) guidelines issued by the American Society of Clinical Oncology (ASCO) now include the use of direct oral anticoagulants (DOACs) for patients with cancer as a preventive measure against VTE recurrence.
To develop the new guidelines, an Expert Panel reviewed 35 publications from 2014 through 2018 focusing on VTE prophylaxis and treatment with 26 categorized as metaanalyses and 9 as randomized controlled trials. The panel reviewed 18 publications that presented VTE risk assessment models.1 “The current update was comprehensive, given the abundance of new evidence basedon recently completed randomized controlled trials of the DOACs for either treatment or prophylaxis,” Gary H. Lyman, MD, MPH, senior lead of health care quality and policy at the Hutchinson Institute for Cancer Outcomes Research in Seattle, Washington, told OncologyLive® in an email.
Included in the review were results of clinical trials that “demonstrate that the new oral agents are at least as active as LMWH [low-molecular- weight heparin] in treating VTE, but some patients are at increased risk for major bleeding,” said Lyman who initiated the creation of the ASCO VTE guidelines in 20072 and served as chair of the Expert Panel committee for over a decade. ASCO issued updates to the guidelines in VTE 2013 and 2015.
Previously, prevention strategies for VTE, which includes deep vein thrombosis (DVT) and pulmonary embolism (PE), were based on the use of LMWH, a class of daily injectable agents. For select high-risk outpatients with cancer, the updated guidelines recommend thromboprophylaxis with one of the new oral agents, apixaban (Eliquis) or rivaroxaban (Xarelto), or an LMWH. In addition, clinicians can consider rivaroxaban and edoxaban (Savaysa) for VTE treatment. Also, patients with brain metastases are now addressed in the VTE treatment selection.1
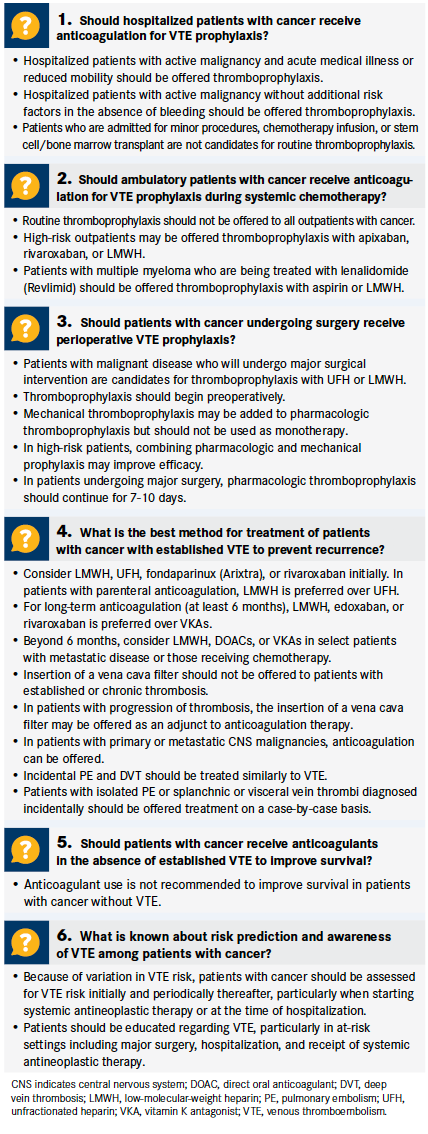
The new guidelines address 6 clinical questions that focus on hospitalized and ambulatory patients, thromboprophylaxis during the administration of systemic chemotherapy, the prevention of VTE recurrence, the use of anticoagulants when patients have no established symptoms of VTE, and the risk prediction and awareness of VTE among patients with cancer (Table 1).1 The guidelines offer recommendations for perioperative VTE prophylaxis in patients undergoing abdominal, pelvic, and other major surgeries who are not at increased risk of bleeding, said Lyman. Clinicians should continue prophylactic treatment until patients are fully ambulatory or longer if they are identified as high risk based on their risk score.
According to the guidelines, the ideal candidate for thromboprophylaxis is a patient who is initiating chemotherapy and at high risk based on a risk score that includes cancer type and high body mass index, and whose baseline blood work indicates elevated white blood cells, elevated platelets, or decreased hemoglobin.1
Patients who are at low risk for VTE or patients at any risk level with a significant chance of major bleeding should not be routinely offered prophylaxis. Further, clinicians need to educate patients about the signs and symptoms of thrombosis, with an emphasis on reporting back any new symptoms or evidence of bleeding.1
“It’s important to personalize or target any of these anticoagulants to patients at greatest risk for VTE and [who are] at lowest risk for bleeding,” said Lyman, also a professor of medicine at the University of Washington School of Medicine in Seattle.
Deep Vein Thrombosis
Between 5% and 10% of patients without a known VTE but who are considered high risk based on their risk score are at risk for blood clots at presentation, either DVT or PE, said Lyman, based on findings from the CASSINI trial, which evaluated rivaroxaban for thromboprophylaxis in high-risk patients.3 He noted that patients who were found to have thrombosis at baseline based on lower-extremity ultrasound were excluded from the CASSINI study. “However, other studies, such as AVERT,4 did not do baseline screening, and presumably some patients who were entered on the trial already had an undiscovered blood clot,” Lyman said.
Table 1. Six Questions and Recommendations About VTE Prevention and Treatment1 (Click to Enlarge)


Risk Model
Table 2. Predictive Model for Chemotherapy-Associated VTE5 (Click to Enlarge)


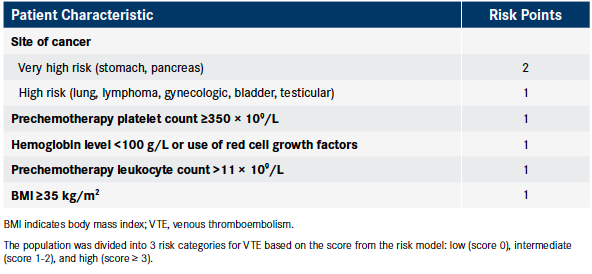
The model was tested in a cohort of 1365 patients, 28 of whom developed VTE. At the cutoff for high risk (score ≥3), the model had a negative predictive value (probabability of of no VTE in those designated low risk) of 98.5%, a positive predictive value (probability of VTE in those designated high risk) of 6.7%, sensitivity (probability of high risk in those experiencing VTE) of 35.7%, and specificity (probability of low risk in those not experiencing VTE) of 89.6% in the validation cohort.5
“The risk model has been integrated into clinical practice guidelines and has been used to select patients for recently completed randomized controlled trials of the DOACs,” said Lyman. “Based on the updated ASCO guidelines, high-risk patients with a Khorana score of 2 or greater, without an increased bleeding risk may be offered thromboprophylaxis with either an LMWH or DOAC. Low-risk patients should not routinely be offered thromboprophylaxis.”
Oncologists should fully evaluate patients with high-risk cancers, such as gastrointestinal, ovarian, and lung, for their overall risk of VTE based on risk score, suggested Lyman. “Prophylaxis may be offered after weighing the risk of bleeding and the benefit of anticoagulation,” he said. “The decision to use thromboprophylaxis should be based on an open discussion between the patient and the treating oncologist after considering those benefits and risks.”
References
- Key NS, Khorana AA, Kuderer NM, et al. Venous thromboembolism prophylaxis and treatment in patients with cancer: ASCO clinical practice guideline update. J Clin Oncol. 2019:JCO1901461. doi: 10.1200/JCO.19.01461.
- Lyman GH, Khorana AA, Falanga A, et al: American Society of Clinical Oncology guideline: recommendations for venous thromboembolism prophylaxis and treatment in patients with cancer. J Clin Oncol. 2007;25:5490-5505.
- Khorana AA, Soff GA, Kakkar AK, et al; CASSINI Investigators. Rivaroxaban for thromboprophylaxis in high-risk ambulatory patients with cancer. N Engl J Med. 2019;380(8):720-728. doi: 10.1056/NEJMoa1814630.
- Carrier M, Abou-Nassar K, Mallick R, et al; AVERT Investigators. Apixaban to prevent venous thromboembolism in patients with cancer. N Engl J Med. 2019;380(8):711-719. doi: 10.1056/NEJMoa1814468.
- Khorana AA, Kuderer NM, Culakova E, Lyman GH, Francis CW. Development and validation of a predictive model for chemotherapy- associated thrombosis. Blood. 2008;111(10):4902- 4907. doi: 10.1182/blood-2007-10-116327.
Clinicians can consider primary prophylaxis in patients with cancer who are initiating chemotherapy and considered high risk based on a validated risk model in the absence of increased risk of major bleeding. The most commonly used risk model was developed by Khorana et al.5 Investigators identified 5 clinical and laboratory parameters that were combined into a simple risk assessment model that allowed providers to classify patients into discrete categories—low, intermediate, and high risk—corresponding to the odds of developing chemotherapy-associated VTE (Table 2).5
It is common for unsuspected blood clots to be detected at the time of routine baseline staging imaging, such as during CT scans, said Lyman. “Those patients should be treated for their VTE with therapeutic doses of anticoagulation. Whether all patients without symptoms should be screened with baseline ultrasounds remains controversial and variable in practice. It would seem reasonable to offer baseline screening ultrasounds to high-risk patients based on their risk score. However, the limited benefit and increased cost probably do not justify routine screening to non—high–risk patients.”



































