
|Videos|July 20, 2020
Antibody Drug Conjugates for Ovarian Cancer
Advertisement
Episodes in this series
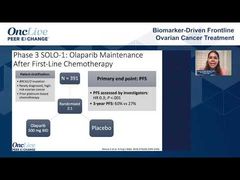















Bradley Monk, MD, FACOG, FACS: In the short time left, let’s talk about some of the new treatments. Clearly when a patient gets recurrent ovarian cancer, the chance of dying is virtually assured. One of these emerging categories, Michael, is antibody drug conjugates. You know we’ve talked about antiangiogenics; we’ve talked about PARP inhibitors, talked about IO [immunotherapy]. The fourth category is antibody drug conjugates. Tell us about what’s in the development phase.
Michael J. Birrer, MD, PhD: You put it the right way; this is a whole new class of drugs. It’s been around for a while, but the technology has not been all that great. Now it’s arrived, and it’s arrived in ovarian cancer. The poster child right now has been mirvetuximab soravtansine, which is a humanized antibody with a chemotherapeutic payload that is targeted to the folate receptor alpha. The folate receptor alpha is a reasonable, well validated target in ovarian cancer. About 60% to 70% of high-grade serous ovarian cancers express high levels of that target. This antibody binds nicely, delivers its payload, and I personally put probably 50 to 60 patients on this kind of drug. The response rate is real.
There’s been some trouble in developing the drug in terms of its randomized phase 3 trial, but they’re now into a repeat trial. It has legs, but I will point this out: the technology, even in mirvetuximab soravtansine, is a bit old in that there are newer approaches. For that, I would bring to your attention the Mersana Therapeutics drug, which targets a different moiety, NaPi2B, a phosphate transporter overexpressed in about 50% of ovarian cancers.
Their technology allows for multiple payloads on the same antibody, and they can define how many payloads go on each antibody. Both drugs are interesting. We’re going to see some of these get approved, and it’s only going to get better. I’ll finish up to say that not only are they effective, but because they’re targeted, they have a much more limited spectrum of toxicity.
Bradley Monk, MD, FACOG, FACS: They also have a biomarker because you can target the folate receptor and the NaPi2B.
Transcript edited for clarity.
Advertisement
Related to this article

In case you missed any, check out our recap of the episodes of OncLive On Air that aired in June 2026.
Advertisement
Advertisement
Trending on OncLive
1
FDA Grants Fast Track Designation to Pelareorep in Pretreated SCAC
2
PRAME-Directed Therapies Advance Melanoma Treatment Across Clinical Settings
3
Dr Falchi on Critical Unmet Needs and Important Next Steps in DLBCL
4
Olverembatinib Plus Blinatumomab Yields High Early-Phase CR/CRi Rates in R/R Ph+ CML and B-ALL
5