
|Videos|July 20, 2020
Neoadjuvant Therapy Versus Surgery for Ovarian Cancer
Advertisement
Episodes in this series















Bradley Monk, MD, FACOG, FACS: What percentage of patients with advanced ovarian cancer get neoadjuvant chemotherapy? I’m going to see how many patients there are who have an opportunity for surgery because she said there are some who don’t. Give me a number of neoadjuvant chemotherapy cases; what do you think?
Leslie Randall, MD, FACOG: Fifty percent, minimum.
Bradley Monk, MD, FACOG, FACS: Let’s say 50%. If you get neoadjuvant chemotherapy, you’re not eligible for secondary cytoreduction, period.
Leslie Randall, MD, FACOG: Not by those criteria.
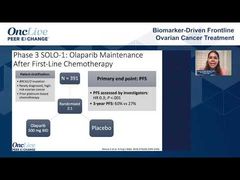
Bradley Monk, MD, FACOG, FACS: We have 3 studies that show no benefit in that because you wouldn’t have been eligible for DESKTOP and SOC-1, and GOG-0213 said it didn’t work. What percentage are R0 [negative resection margin] out of the 50%?
Leslie Randall, MD, FACOG: If we’re talking interval debulking….
Bradley Monk, MD, FACOG, FACS: No, frontline debulking.
Leslie Randall, MD, FACOG: That’s right. I was going to say you’re excluding those outright, right? Primary debulking, R0, 50%.
Bradley Monk, MD, FACOG, FACS: You’re now down to 25% who are at least eligible.
Leslie Randall, MD, FACOG: These are smart people; are these fair numbers?
Bradley Monk, MD, FACOG, FACS: Yes, of course they are.
Shannon N. Westin, MD, MPH, FACOG: They seem reasonable.
Bradley Monk, MD, FACOG, FACS: I think so. Right out of the gate, 75% of the patients don’t talk about it because they weren’t…primary debulking, and they didn’t have an R0. Then what’s the percentage of patients who are going to have a platinum-resistant recurrence because you have to have platinum-sensitive recurrence? Let’s say 20%. Now you go from 25% to 20%, and then what percentage of patients are going to have these isolated recurrences that you can resect?
Leslie Randall, MD, FACOG: Probably about a quarter or a third of patients.
Bradley Monk, MD, FACOG, FACS: Yes, so let’s say a third. A third of 20% is about 5% to 10%. That’s OK; I’m not going to fight you.
Leslie Randall, MD, FACOG: That’s OK. I’m refereeing because you told me to. That’s OK because we’re looking for the people who shouldn’t have surgery, right?
Bradley Monk, MD, FACOG, FACS: Yes.
Leslie Randall, MD, FACOG: That’s a good algorithm to go through, in my opinion.
Bradley Monk, MD, FACOG, FACS: Thank you for that. What happens, I’m afraid, is that, as Dr Pinkal Desai, [MD, MPH,] who was Dr Randall’s and our mentor, said, “When you’re a hammer, all the world is a nail. And when you’re a surgeon, you’re looking for someone to operate on.”
Leslie Randall, MD, FACOG: He also said, “A good surgeon knows when to operate, and a great one knows when not to.”
Bradley Monk, MD, FACOG, FACS: Thank you. That’s good wisdom; that’s fantastic wisdom.
Transcript edited for clarity.
Advertisement
Related to this article

In case you missed any, check out our recap of the episodes of OncLive On Air that aired in June 2026.
Advertisement
Advertisement
Trending on OncLive
1
FDA Grants Fast Track Designation to Pelareorep in Pretreated SCAC
2
PRAME-Directed Therapies Advance Melanoma Treatment Across Clinical Settings
3
Dr Falchi on Critical Unmet Needs and Important Next Steps in DLBCL
4
Olverembatinib Plus Blinatumomab Yields High Early-Phase CR/CRi Rates in R/R Ph+ CML and B-ALL
5