
|Videos|July 20, 2020
New Data for Secondary Surgery in Ovarian Cancer
Advertisement
Episodes in this series
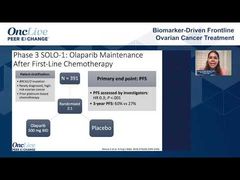















Bradley Monk, MD, FACOG, FACS: Matt and Shannon, I want to pivot here to the other most important abstract. I would say at ASCO [the American Society for Clinical Oncology annual meeting], the No. 1 and No. 2, I’m not sure one is better than the other, but that SOLO-2 overall survival [OS]; and maybe it’s not the most important because it’s not going to change practice. Let’s get into the secondary debulking conversation.
There was a study published in The New England Journal of Medicine that many of our listeners may have participated in called GOG-0213. It showed that a second operation wasn’t helpful. Tell us about that study, Matt.
Matthew Powell, MD: We talked a little about GOG-0213 just a bit ago when we were talking about chemotherapy selection. This was a bit complicated because it was both a chemotherapy question and a surgical question that was asked. Part of the reason Rob Coleman, [MD,] has gray hair is mostly this trial.
There were 485 patients randomized; 67% of them had complete gross resection. Follow-up was good for the trial. Most of these patients had bevacizumab, which is the main difference from the other trial; 84% of the patients had bevacizumab. The hazard ratio favored the group for which you didn’t operate: 1.3. It was a year longer if you didn’t operate on them, from an OS standpoint. We scratched our heads after this trial came out.
There was definitely some patient selection that ended up being part of the randomization. The surgical morbidity was about what we expected. We anxiously awaited DESKTOP 3, and Shannon’s going to tell us about that.
Bradley Monk, MD, FACOG, FACS: It’s interesting. I always say it takes 2 studies to convince anyone of anything. I don’t know why you guys have adopted the LACC trial with 1 study. The LACC trial was a cervical cancer trail that showed that if you have radical hysterectomy, open, you live longer than if it was minimally invasive. GOG-0213 didn’t change practice; it changed opinions a bit. The second, confirmatory trial was supposed to be DESKTOP 3, and that was presented at ASCO. Did it confirm or refute GOG-0213? Shannon, tell us.
Shannon N. Westin, MD, MPH, FACOG: Well it’s a little complicated.
Bradley Monk, MD, FACOG, FACS: It did both.
Shannon N. Westin, MD, MPH, FACOG: It’s a little bit of both, right? It was a nicely designed study, and to Matt’s point, they were a bit stricter around the selection of the patients. They used their AGO [German gynecological oncology group] model that they had previously validated in other studies that includes looking at ECOG performance status, were they able to get to no gross residual disease after surgery the first time? Did they have ascites at recurrence?
They randomized patients based on if they met these criteria to either secondary cytoreduction or going directly to chemotherapy. They all got platinum-based chemotherapy. There was no mandate to include any other targeted therapies. In this study, about 22% to 23% of patients on each arm received bevacizumab. There was only a smaller population that had the chemotherapy with that drug, which we know can be a great equalizer between groups.
What they found was a significant difference in progression-free survival, which was one of the co-primary end points. We all thought, “That’s great; the tumor’s been resected, so of course it’s going to take longer for you to see something and progress. What we really want to see is overall survival.” That’s what they presented at ASCO this year, and they demonstrated a statistically significant and clinically significant difference in overall survival, with a reduction in the risk of death of about 25%, a hazard ratio of 0.75. That yielded about a 7-month difference in overall survival.
When they teased out the patient populations, that’s where things got interesting. The patients for whom the surgeon was able to achieve no gross residual did by far the best. The median was somewhere around 62 months for those patients.
Bradley Monk, MD, FACOG, FACS: GOG-0213 showed that too, that could be biology.
Shannon N. Westin, MD, MPH, FACOG: That’s right, but when you look at the population that got surgery and did have residual disease, they did worse than the chemotherapy alone arm. This told me that we need to do a better job of knowing how to select these patients. We all, the surgeons here, we all have patients in our practice for whom we did secondary cytoreduction who lived another 6 or 7 years, and we high-five ourselves, but you’re right, it’s the biology. We need to do a better job of selecting them.
For me, this says that there is a population that we should not operate on. And there’s a population that can potentially benefit from surgery. Where does bevacizumab add into that? Does that negate the surgery, and if you’re going to give bevacizumab, then it doesn’t matter? We’re still trying to understand it.
The other abstract that was presented at ASCO, the SOC-1 trial, which was a study that had a similar population; they did a bit different selection. They had a score that they utilized called the iMODEL that incorporates things like stage. Were they able to get R0 [negative resection margin] after their primary cytoreduction? What is the CA-125 [cancer antigen 125] level? Ascites?
In that group, they did not demonstrate a benefit in overall survival. We saw progression-free survival benefits for the patient population that got surgery, but they did not demonstrate a statistically significant difference in overall survival in that group. It’s still early, but it’s again a bit confusing.
When you look at the curves, it’s the same thing. The population that can get that R0, benefits. The population that gets surgery but does not get to no gross residual disease looks worse than the population that gets chemotherapy.
Bradley Monk, MD, FACOG, FACS: In GOG-0213, the no surgery did better than the R0.
Transcript edited for clarity.
Advertisement
Related to this article

In case you missed any, check out our recap of the episodes of OncLive On Air that aired in June 2026.
Advertisement
Advertisement
Trending on OncLive
1
FDA Grants Fast Track Designation to Pelareorep in Pretreated SCAC
2
PRAME-Directed Therapies Advance Melanoma Treatment Across Clinical Settings
3
Dr Falchi on Critical Unmet Needs and Important Next Steps in DLBCL
4
Olverembatinib Plus Blinatumomab Yields High Early-Phase CR/CRi Rates in R/R Ph+ CML and B-ALL
5