
|Videos|July 20, 2020
Treating Homologous Recombination Proficient Ovarian Cancer
Advertisement
Episodes in this series















Bradley Monk, MD, FACOG, FACS: In the HRP [homologous recombination proficient] subset, we have to decide if it is PARP inhibition alone, as you just said Leslie, or is it bevacizumab alone? You can’t give both. How do you look at that? I would even put it out there: let’s not do the biomarker. I know there’s all this controversy. The biomarker is important; it’s a CDx [companion diagnostic].
Matt, how do you look at this HRP patient? I get it it’s the highest unmet need. I get it that that’s where research really needs to be done. What’s the best treatment for the HRP patient, and how do you make that decision?
Matthew Powell, MD: Wow, why do you keep asking me all these hard questions?
Bradley Monk, MD, FACOG, FACS: Because you’re the smartest guy.
Matthew Powell, MD: That’s far from true…. That’s the patient who has no real targetable options. Maybe they have bevacizumab as an advantage. We’re going to spend a lot more effort thinking about what to do with these proficient patients, or the patients who had an HRD [homologous recombination deficient] scar who is no longer deficient, who has reactivation of their homologous recombination pathway. Those patients are out there as well.
What we did learn is that HRD is not perfect. We learned from the VELIA trial that the assays, wherever we draw these lines, are really tricky. The nice part about it is that, in the recurrent setting, we have patients who responded to platinum twice, and I can see that patient’s probably a PARP inhibitor candidate. If you barely responded to platinum the first time, it’s hard to know what to do with that patient; we don’t have great options for those people.
Bradley Monk, MD, FACOG, FACS: One of the best things about being in education is what I call reverse mentorship. I said Leslie Randall was my fellow, and now I’m her trainee. What she just said here is very impactful. What she said, if I’m interpreting you correctly, Leslie, is that this may be the only chance for that HRP patient to get a PARP Inhibitor.
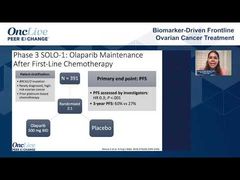
There’s a chance, just as you said Matt, that she’s going to have a platinum-sensitive relapse. The medium time to progression with HRP is 5.4 months in PRIMA. Half of them for sure are going to be platinum-resistant. The other half may have a platinum-sensitive relapse, but they then have to respond; remember, they’re HRP, so the chance of responding to platinum again is low.
Does that resonate with you Shannon, that it may be that the HRP patient should get a PARP inhibitor? In this case, it’s niraparib. Biomarkers are not perfect, and there are some patients who even have HRP who can do well for a long time on a PARP inhibitor. What do you think about that?
Shannon N. Westin, MD, MPH, FACOG: I’ve had this conversation now several times with patients in the clinic where they want to do something. We’ve done the testing on the tumor; the tumor is apparently HR-proficient, but that’s exactly what I say, “This is not a perfect test. There was clearly a proportion of patients who were identified to be HR-proficient who had benefit from the PARP inhibitor. I don’t know who they are, and you might be one, so if you’re willing, and you want to do something, then this is an extremely reasonable thing to do.” The elephant in the room here is that we’re all eagerly anticipating what the results of all these new combination trials that are ongoing and accruing will be in that patient population. We had hoped that PAOLA would be positive in the HR-proficient, but here we are.
Bradley Monk, MD, FACOG, FACS: I want our audience to notice, they’re like athletes; they have game faces. I love it when Shannon starts to talk to me like her patient. She gets to wear her game face.
Shannon N. Westin, MD, MPH, FACOG: It’s true.
Bradley Monk, MD, FACOG, FACS: I thank you; that shows your passion.
Transcript edited for clarity.
Advertisement
Related to this article

Experts convened to discuss ADC sequencing strategies, biomarker testing infrastructure, and emerging data across cervical, ovarian, and endometrial cancers.

The top 5 OncLive TV videos of the week cover insights in breast cancer, lymphoma, melanoma, prostate cancer, and ovarian cancer.

The FDA accepted for review a sBLA for subcutaneous mosunetuzumab plus polatuzumab vedotin in LBCL, a BLA for ozekibart in chondrosarcoma, and more.

Did you catch all of this week's top oncology news? Test your knowledge with OncLive's Weekly News Quiz.
Advertisement
Advertisement
Trending on OncLive
1
SERENA-6 Controversies Push the Breast Cancer Field to Consider the Future Role of ctDNA-Guided Treatment Decisions
2
FDA Approval Positions Belzutifan Plus Pembrolizumab as a New Adjuvant Standard in ccRCC
3
June’s GI Rewind: CRC, Gastric Cancer See Several “Firsts” With FDA Review of Adjuvant IO, Global Approval of BRAF-Targeted and CAR T-Cell Therapies
4
SYNC-T SV-102 Employs Novel Mechanism to Target Immunologically ‘Cold’ Tumors in Advanced Metastatic Prostate Cancer
5