
|Videos|February 1, 2018
Diarrhea Prophylaxis With Neratinib
Advertisement
Episodes in this series













Transcript:
Debu Tripathy, MD: This is a big question: Should we be using diarrhea prophylaxis? I think that if you use diarrhea prophylaxis, you are going to have less diarrhea. I have used that for quite some time with my patients, both with pertuzumab as well as with neratinib. However, we have also learned that if you take that approach, some patients will actually have constipation. Another approach that I sometimes use for my patients, depending on whether they’re naturally prone to constipation or diarrhea, is to not take it prophylactically but take it steadily to the first bowel movement, then take a double dose, and then take it every 6 hours. We do tell patients not to take more than 12 2-mg tablets a day. That way, they can stay on top of it. Sometimes we use drugs like Lomotil [atropine/diphenoxylate]. There is a nonrandomized study looking at diarrhea control called the CONTROL study that is testing a variety of other drugs, such as bile-sequestering agents like colestipol, and nonabsorbable steroids have also been tried. It looks like the bile-sequestering agents might be the most effective, at least with the preliminary data that have been presented so far. But we need a little more information and follow-up to solidify those recommendations.
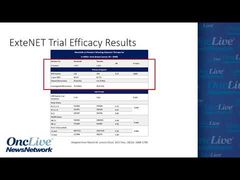
Ruta D. Rao, MD: When starting neratinib, diarrhea prophylaxis should strongly be considered. Based on the CONTROL trial, we can say that loperamide with either budesonide or colestipol, or both, should be used. You can see that the results were significantly improved for the rates of diarrhea compared with the ExteNET trial, in which no prophylaxis was mandated.
Transcript Edited for Clarity
Advertisement
Related to this article

Catch up on insights into the global development of breast cancer treatments in the global spotlight.

Dato-DXd was approved in the European Union as monotherapy for patients with first-line metastatic TNBC who are not candidates for immunotherapy.

The FDA issued final guidances on performance status, washout periods, and laboratory values aimed at expanding oncology trial participation.

The FDA accepted an NDA for daraxonrasib in metastatic pancreatic cancer, approved zidesamtinib in pretreated ROS1-positive NSCLC, and more.

The CHMP recommended EU approval of T-DXd plus pertuzumab as first-line therapy for HER2-positive metastatic breast cancer,

The CHMP has recommended the approval of sacituzumab govitecan/pembrolizumab for treatment-naive, PD-L1-positive metastatic TNBC in the European Union.

Watch a highlight reel of breast cancer data from ASCO 2026 that experts anticipate will have the biggest impact on the field.
Camizestrant plus a CDK4/6 inhibitor was approved in the European Union for ER-positive, HER2-negative advanced breast cancer with an emergent ESR1 mutation.
Advertisement
Advertisement
Trending on OncLive
1
FDA CTGTAC Votes in Favor of RP1/Nivolumab Data in Advanced Melanoma
2
Dr Barot on the FDA Approval of Palbociclib/Trastuzumab ± Pertuzumab in HER2+ Breast Cancer
3
Dana-Farber Researchers Identify CDK8 as a Potential Therapeutic Target for Alveolar Rhabdomyosarcoma
4
Dr Galsky on Data Supporting the FDA Approval of Perioperative EV/Pembrolizumab in MIBC
5