
|Videos|July 20, 2020
Emerging Combinations in the Frontline Setting of Ovarian Cancer
Advertisement
Episodes in this series
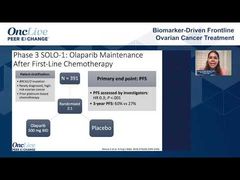















Bradley Monk, MD, FACOG, FACS: In the last few minutes in our conversation about frontline ovarian cancer, let’s go ahead and talk about combinations. I only want to spend about 30 seconds per study, and this will be brief. Matt, I want to take you to the first one, which has already been published. It is a combination with chemotherapy, but it’s not labeled. Tell us about VELIA.
Matthew Powell, MD: VELIA was a very large study, 1000-plus patients studied, looking at the idea of using veliparib, which is a PARP inhibitor that you can combine with chemotherapy without too much toxicity. It’s lower dose, can be combined with carboplatin-paclitaxel, and then given as a maintenance therapy.
Cutting to the chase, the take-home message is that it didn’t seem to matter if you combined it with chemotherapy. It didn’t seem to help that much more than what we already have. Do we need a fifth PARP inhibitor? I’m not sure. I will say that it will attempt the FDA approval, but I’m not sure there’s a lot of interest beyond what we already have.
Bradley Monk, MD, FACOG, FACS: Another combination obviously is PARP/IO immunotherapy. There’s a study called ATHENA, which adds rucaparib, a PARP inhibitor we haven’t talked about much. It adds rucaparib to nivolumab, with 400 patients in each arm. It takes the PRIMA indication of single-agent PARP inhibitor, in this case rucaparib, and adding an IO to it, niraparib, which will be interesting. The other part of that study though is indeed the PRIMA study, where placebo was compared to niraparib.
There will be 2 readouts from ATHENA; one PRIMA-like with rucaparib versus placebo, and that will come first. The other one, which will be beyond, or sort of ATHENA2, will take the single-agent PARP inhibitor with nivolumab, so I’m excited about that. Then the obvious question, Shannon, is triplet therapy. Maybe we should add bevacizumab, IO, and a PARP inhibitor. There are 3 studies looking at that.
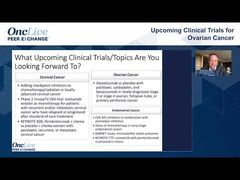
Shannon N. Westin, MD, MPH, FACOG: Yes there are, and they’re pretty similar. The first study is taking an upfront population. They get a cycle of chemotherapy while they’re obtaining stratification factors, and then they’re randomized to 3 arms. There’s a chemotherapy alone arm, which can include bevacizumab. Then there’s the chemotherapy followed by a PARP inhibitor maintenance with niraparib, and again, bevacizumab can be included on that.
Finally, there’s a chemotherapy with dostarlimab, a checkpoint inhibitor, with or without, and then including the niraparib. There are 3 arms, so we’re going to get an idea of PARP inhibitor, PARP/IO, and then bevacizumab is included per investigator choice throughout those 3.
There are 2 trials looking at combinations with olaparib. DUO-O is looking at the same population’s response either pre- or post-surgery. They get randomized to chemotherapy with or without durvalumab, and then with or without olaparib as a maintenance. Similarly, ENGOT-OV46 is looking at a similar population with pembrolizumab instead of durvalumab. Importantly, DUO-O allows for bevacizumab, and then ENGOT-OV46 is simply the olaparib/pembrolizumab question.
Bradley Monk, MD, FACOG, FACS: It’s interesting. Matt, to your point with VELIA, do we need a fifth PARP inhibitor because talazoparib is approved in breast cancer? You can see that there are 6 checkpoint inhibitors approved. Dostarlimab, which you talked about, will be number 7, and not only is dostarlimab integrated into this triplet opportunity, but so are durvalumab and pembrolizumab. It’s a competitive landscape. The real opportunity here, I can’t remember which of you said it, is in the HRP [homologous recombination proficient] population.
We have a 0.43 hazard ratio in PAOLA-1 in the HRD [homologous recombination deficient] subset with a doubling of the PFS [progression-free survival]. You don’t even get the doublet bevacizumab/olaparib in HRP. Even in PRIMA where HRP is labeled, it doesn’t work well. I’m excited about that opportunity.
I’m going to ask each of you for a closing comment: what you’re excited about moving forward as this rolls out, as we complete our conversation about frontline ovarian cancer. Leslie, why don’t you go ahead and tell us what you’re excited about as a last comment in our frontline discussion.
Leslie Randall, MD, FACOG: I’m excited to have options. I’m excited to have PARP inhibitors outside of BRCA for sure. Trying to decide who is getting bevacizumab, I’m biased toward bevacizumab, I use a lot of it as well, so trying to decide who’s going to be best for that combination moving forward, is where I’m still working.
Bradley Monk, MD, FACOG, FACS: Dr Birrer, as we finish this conversation about frontline, newly diagnosed ovarian cancer, what are your closing comments?
Michael J. Birrer, MD, PhD: I share what Leslie said. It’s an exciting time for our patients. Having survived the IP [intraperitoneal] versus IV [intravenous] debate, we’re in a much better period, so it’s exciting. We need to settle this issue as to whether IO works, in particular if it works up front. By testing it up front, we can avoid that issue about when the tumors are all beat up and the immune system is beat up. We need to settle that, and I remain optimistic that it may not be a single agent like JAVELIN 100, but it may be a combination, antiangiogenic plus IO.
Bradley Monk, MD, FACOG, FACS: As you know, JAVELIN 100 was just avelumab and chemotherapy. To your point, we didn’t review that negative study, which was presented at the SGO [Society of Gynecologic Oncology annual meeting] by Jonathan Ledermann BSc, MD, FRCP. It didn’t seem to benefit. If anything, it may have been a little hurtful, although you can’t make that conclusion.
Matt, what are your closing remarks?
Matthew Powell, MD: Two things. One is that we learned a few things during COVID-19 [coronavirus disease 2019]. We’re much more aggressive using neoadjuvant chemotherapy. I don’t think we’re hurting our patients. The value of the knife is going down. We just reviewed our fellowship data, we’re doing much less radical surgery than we used to, and our patients are doing better, which is quite exciting. I’d like to be put out of a job as an oncologist, but we need to learn how to use these new tools the best. With all these targeted therapies, I hope they’re helping our patients.
Bradley Monk, MD, FACOG, FACS: To your point, historically, only about half of gynecologic oncologists give systemic therapy. Who gives the treatments? The medical oncology community. I’m honored that the medical oncology community is engaged in these conversations. Quite frankly, I think they do a very nice job. Moving forward, we have to teach our fellows, as you just outlined, beyond surgery because the surgery isn’t changing. The systemic therapy is. Shannon, you have the last word.
Shannon N. Westin, MD, MPH, FACOG: In this group, it’s hard because I agree with everybody. I’m excited. We have many options that we’ve gotten over the last few years. It’s thrilling, but it’s like drinking through a firehose at times trying to make those decisions about which things we want to give what patient. I’m excited about the results that are going to read out over the next few years from these combination trials, and I remain hopeful that we’ll continue to tease out the HRD test to help it better select our patients.
Bradley Monk, MD, FACOG, FACS: I want to thank my panel. I want to thank Dr Randall, Dr Birrer, Dr Westin, and Dr Powell. On behalf of OncLive®, thank you so much for being with us, and so long for now.
Transcript edited for clarity.
Advertisement
Related to this article

In case you missed any, check out our recap of the episodes of OncLive On Air that aired in June 2026.
Advertisement
Advertisement
Trending on OncLive
1
FDA Grants Fast Track Designation to Pelareorep in Pretreated SCAC
2
PRAME-Directed Therapies Advance Melanoma Treatment Across Clinical Settings
3
Dr Falchi on Critical Unmet Needs and Important Next Steps in DLBCL
4
Olverembatinib Plus Blinatumomab Yields High Early-Phase CR/CRi Rates in R/R Ph+ CML and B-ALL
5