
|Videos|February 1, 2018
Factors Influencing Adjuvant Therapy Use for HER2+ Breast Cancer
Advertisement
Episodes in this series













Transcript:
Ruta D. Rao, MD: There are a number of factors that we take into account when we decide which adjuvant regimen to use, and these would include nodal status, tumor size, and hormone receptor status specifically. For patients who have small tumors that are node-negative, there have been great efficacy results from a phase II trial looking at Taxol [paclitaxel] and trastuzumab in these patients: 12 weeks of weekly Taxol with a year of trastuzumab. The 7-year disease-free survival from this trial reported by Sara Tolaney was 93.3%. That’s a very acceptable regimen for patients who have small tumors and were lymph node—negative. Specifically, in that trial, the tumors were less than 3 cm.
Residual disease after neoadjuvant therapy is an important prognostic factor. We know that for HER2-positive patients, the amount of residual disease after their neoadjuvant therapy correlates with their prognosis and risk of distant recurrence. I don’t use that specifically to determine which regimen to use because those patients have already received their neoadjuvant chemotherapy regimens.
There are some patient factors that I would take into account when thinking about which regimen to give a patient, specifically what their cardiac risk is. We know that women who are older and who have cardiac risk factors may have an increased risk of cardiac events if an anthracycline-based regimen is used.
Debu Tripathy, MD: I think that one can use the same criteria for both decisions because it really boils down to, How much risk does the patient have? If the patient has started with surgery, then I think you use the standard staging criteria. You use lymph nodal involvement, which is the first and most important. For node-negative disease, I’d go by tumor size and grade. Generally, with a tumor that’s a higher grade and more than 1 cm, I think the risk is high. There are going to be those gray areas. For example, a patient with a 1-cm tumor but who is grade 2—that can be a wash. But for someone with a 0.7-cm tumor and grade 1 hormone receptor—positive disease, I don’t think there’s much to be added from pertuzumab. I think that’s the guidance I would use.
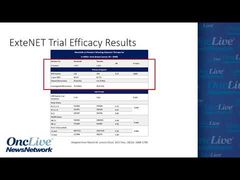
Now, I think the decision about using pertuzumab and neratinib is not necessarily dependent or either/or. You could potentially use both. We don’t have much data, of course, because the ExteNET study really was in the pre-pertuzumab era and all those patients received trastuzumab. That was the requirement to go on that study, but that study showed similar findings, as do most. If the study is positive, the absolute benefit is going to be greater in patients who have higher-risk features to start with, either residual disease after neoadjuvant therapy or positive nodes, a large mass, or higher-grade disease. If one is using pertuzumab as the antibody added to trastuzumab for very high-risk disease, let’s say for positive lymph nodes, then it would stand to reason that following the completion of antibody therapy, which is typically when you’d start neratinib, the patient would be a good candidate for neratinib, as well, because they still have a higher residual risk.
Now, this is assuming that there isn’t an interaction between pertuzumab and neratinib, that if for some reason you receive pertuzumab and have a better outcome, that all of a sudden negates the benefit of neratinib. There’s no reason a priori to expect that would be the case. So I think that those are independent decisions. If you think the patient is high risk, they can get both. The ExteNET study you will hear about in more detail later did suggest that the benefit was higher in hormone receptor—positive disease, and some may assume that can be used as a decision point for treating patients. That may be the case, but I think if you look at it rigorously, the statisticians will tell you that the study wasn’t designed to really look specifically at that. I don’t think we should routinely be using that. But the important point to make here is that these are independent decisions. You could get neither of the additional HER2-targeted therapies, you might be recommended for both, or you might be at the midway point, where only one of them is used.
Ruta D. Rao, MD: Based on the NeoSphere data, I use a regimen with trastuzumab, pertuzumab, and chemotherapy in the neoadjuvant setting, specifically for patients who have node-positive disease and tumors larger than 2 cm and who present with locally advanced disease or inflammatory breast cancer. In the adjuvant setting, I would consider using pertuzumab in addition to trastuzumab for patients who I perceive to be at a higher risk of recurrence, specifically if they were estrogen receptor—negative and had multiple lymph nodes involved with their tumor.
Based on the ExteNET trial, the patients who would seem to benefit the greatest from adjuvant neratinib after completing a regimen of adjuvant trastuzumab for a year were those who had high risk of recurrence, specifically node-positive disease and hormone receptor—positive disease. So I would consider using it in a patient like that.
Transcript Edited for Clarity
Advertisement
Related to this article

Catch up on insights into the global development of breast cancer treatments in the global spotlight.

Dato-DXd was approved in the European Union as monotherapy for patients with first-line metastatic TNBC who are not candidates for immunotherapy.

The FDA issued final guidances on performance status, washout periods, and laboratory values aimed at expanding oncology trial participation.

The FDA accepted an NDA for daraxonrasib in metastatic pancreatic cancer, approved zidesamtinib in pretreated ROS1-positive NSCLC, and more.

The CHMP recommended EU approval of T-DXd plus pertuzumab as first-line therapy for HER2-positive metastatic breast cancer,

The CHMP has recommended the approval of sacituzumab govitecan/pembrolizumab for treatment-naive, PD-L1-positive metastatic TNBC in the European Union.

Watch a highlight reel of breast cancer data from ASCO 2026 that experts anticipate will have the biggest impact on the field.
Camizestrant plus a CDK4/6 inhibitor was approved in the European Union for ER-positive, HER2-negative advanced breast cancer with an emergent ESR1 mutation.
Advertisement
Advertisement
Trending on OncLive
1
FDA CTGTAC Votes in Favor of RP1/Nivolumab Data in Advanced Melanoma
2
Dr Barot on the FDA Approval of Palbociclib/Trastuzumab ± Pertuzumab in HER2+ Breast Cancer
3
European Commission Approves First-Line Dato-DXd for Immunotherapy-Ineligible Metastatic TNBC
4
Dr Galsky on Data Supporting the FDA Approval of Perioperative EV/Pembrolizumab in MIBC
5