
|Videos|July 20, 2020
Impact of HRD Status on Frontline Treatment of Ovarian Cancer
Advertisement
Episodes in this series
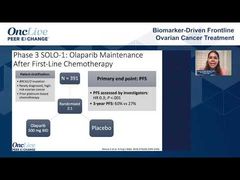















Bradley Monk, MD, FACOG, FACS: Leslie, about the biomarkers, there are a lot of conversations about this HRD [homologous recombination deficiency] biomarker. We should try to keep it simple. I realize that the biomarker is not perfect. At least tell us what the biomarker was both in PRIMA and PAOLA.
Leslie Randall, MD, FACOG: The biomarker is called HRD. I call it a phenotypic assay of DNA repair deficiency, homologous recombination deficiency. It has a score that has 3 components: loss of heterozygosity [LOH], telomeric allelic imbalance, and a large-scale state transition. They then give you a score of which somatic BRCA is a part. The scoring is complicated, and if you’re interested, I would have you look at the package insert for the Myriad Genetics, Inc myRisk test, but the cutoff is generally set at 42.
Bradley Monk, MD, FACOG, FACS: MyRisk is germline, myChoice is somatic.
Leslie Randall, MD, FACOG: Right, myChoice. I misspoke, thank you for correcting me. The cutoff for PRIMA and PAOLA is set at 42. You don’t have to set the cutoff at 42. That’s not been stringently validated; it’s just a cut point that we’ve chosen to use. There are things that are not measured in the myChoice test that contribute to HRD, and we don’t know the exact cutoff yet, so it’s not yet a perfect test. But if you look at the totality of all this frontline data, it’s pretty discriminatory with regard to the outcome. Although we say it’s not a perfect biomarker, it’s not an imperfect biomarker by any means. It can be very helpful in an upfront setting.
Bradley Monk, MD, FACOG, FACS: Because it’s a companion diagnostic for PAOLA-1, as Matt said, it is reimbursed by CMS [Centers for Medicare & Medicaid Services] and others. There is a second commercially available option. You said it nicely: it’s a functional test. Looking at the mutation is not acceptable. The other functional test is Foundation Medicine, Inc’s LOH test. Is that as good, Michael Birrer? I know you’ve spent a lot of your career on this biomarker. Should we stick with the companion diagnostic because we don’t want to interfere with the reimbursement? How do you integrate the Myriad myChoice with the Foundation LOH score?
Michael J. Birrer, MD, PhD: You just hit on it. It’s more of a reimbursement insurance issue. If you look at fundamentally how the assays were developed, they’re both based on LOH. Myriad just added those 2 other elements that Leslie talked about. I’m not sure how much they add, but I tend to agree; the assay works. It’s not perfect. Hopefully with more research, we’ll get it better and more accurate, but I remind all of my colleagues, even estrogen receptor expression doesn’t predict a tamoxifen response in breast cancer all the time. No biomarker is perfect.
Bradley Monk, MD, FACOG, FACS: Matt, we’re all friends, but I’m going to ask you one of the toughest questions of the day, and I’m sorry. When I look at PRIMA versus PAOLA, 2 very impactful frontline trials, I see, as Leslie very nicely said, that there was an impact in the HRP [homologous recombination proficient] group, in other words the non-HRD group. I didn’t see that in PAOLA.
I want to explore that. I know we’re not going to get to the answer, but these are the questions that everyone is asking. What is the reason that there was no benefit in PAOLA-1 in the HRP subset? I’m going to give you some choices, or maybe there’s another answer. Is it because niraparib works in HRP and olaparib doesn’t? Or is it because the bevacizumab negated the effect of olaparib? Maybe olaparib performed as well as niraparib in HRP and bevacizumab negatively affected that? Or is it something else?
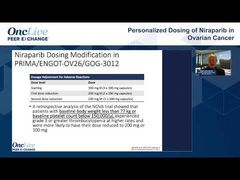
Matthew Powell, MD: Without a head-to-head comparison, we won’t know. That is the tricky part here. The dose might matter in the proficient population, and we are probably getting a little better dose or penetration to the tumor with niraparib. Perhaps it’s that slight difference; maybe they’re the same as far as PARP inhibition, but we can get a better dose in the patients who are wild type or are HR proficient.
Both things are probably in effect. The bevacizumab is helping the placebo arm to do better in negating the effects of what we see with olaparib in PAOLA. I don’t know the answer. It’s nice that we have an option for PARP inhibition in our proficient patients. I’ll leave it at that and say, “Thank you, FDA, for giving us some choices.”
Bradley Monk, MD, FACOG, FACS: Shannon, I want everyone’s opinion on this because this is what our audience wants to know, and it’s what I want to know. This is not meant to be a commercial; I’m not trying to sell anybody anything. I’m trying to help patients. I get that I’m a coauthor in many of these papers, and I don’t want that to influence my opinion. That’s why I’m going to let you talk.
Niraparib is the only PARP inhibitor in treatment. We’re going to talk about it and proof beyond BRCA. These are just the facts. Niraparib is in NOVA again in treatment maintenance, the effect was pretty well defined; when in study GOG-219, it was a phase 2 study. Is niraparib’s higher tissue concentration more effective at cytotoxicity? I’m not going to get into the mechanism of action, or do you think these are clinical trial design issues?
Shannon N. Westin, MD, MPH, FACOG: I’ve seen the data around the penetration, and it does give you a sense, but I don’t know that we’ve ever been able to prove that that has any impact on efficacy. These are different populations. The PAOLA patient population is very different than the population from PRIMA, which was more bad actors. Perhaps you’re seeing a difference that may be statistically significant, but how clinically significant is it, based on the patient population?
The other thing is that you’ve got to remember that there’s an active comparator. These patients in PAOLA, they’re not getting placebo. They’re getting bevacizumab, which we know is an active drug. That could potentially impact it. We’ve all had the sense that it seems like the bevacizumab control arm performed a bit better than what we would expect to see. Perhaps that has something to do with it.
With that being said, I’m intrigued by the early overall survival results that were presented at the time with PRIMA, looking toward a hint in that homologous recombination proficient group. I’m eagerly awaiting those results to see if that plays out because that would then potentially indicate that you are getting some more tissue penetration, and you are benefiting a patient with your sequencing and giving that PARP inhibitor earlier in their disease.
Bradley Monk, MD, FACOG, FACS: We get better at these targeted agents. What you said is that bevacizumab did a little better. Why would it do better in PAOLA-1? If you look at the discontinuation rate in GOG-0218, it was about 20%. We’re just learning how to handle the proteinuria and the hypertension, that sort of thing. In PAOLA-1, the discontinuation of bevacizumab was about 5%.
Shannon N. Westin, MD, MPH, FACOG: Right.
Bradley Monk, MD, FACOG, FACS: These agents work only when you use them, and if you can keep patients on treatment longer because you understand the supportive care, there might be a bigger benefit.
Shannon N. Westin, MD, MPH, FACOG: If you design your trial based on what you expect, then it performs. You are right: we are better at it. We’re much better at it, but they designed it based on the prior data, and that impacted the appearance of statistical significance and clinical significance.
Transcript edited for clarity.
Advertisement
Related to this article

In case you missed any, check out our recap of the episodes of OncLive On Air that aired in June 2026.
Advertisement
Advertisement
Trending on OncLive
1
FDA Grants Fast Track Designation to Pelareorep in Pretreated SCAC
2
PRAME-Directed Therapies Advance Melanoma Treatment Across Clinical Settings
3
Dr Falchi on Critical Unmet Needs and Important Next Steps in DLBCL
4
Olverembatinib Plus Blinatumomab Yields High Early-Phase CR/CRi Rates in R/R Ph+ CML and B-ALL
5