
|Videos|July 20, 2020
Personalized Dosing of Niraparib in Ovarian Cancer
Advertisement
Episodes in this series















Bradley Monk, MD, FACOG, FACS: Michael, one of the interesting things about PRIMA is that they changed the dose, they personalized the dose. Tell us about that.
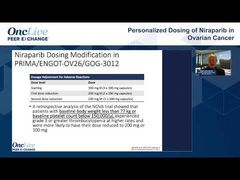
Michael J. Birrer, MD, PhD: The original observation extended from NOVA, where there was not an insignificant amount of thrombocytopenia. We were involved in that trial, and there were patients whose platelet counts went down below 10,000. A retrospective analysis of that study showed that a lot of those patients could be identified because of low body weight, thin habitus, and low platelets, called weights and plates.
When PRIMA was designed, as you know, this was then inserted into what we would call individualized dosing in that trial. Like a lot of things, there’s good news and bad news. The good news is that approach worked. There was much lower incidence of thrombocytopenia. Although I might add that when it was presented at ESMO [the European Society for Medical Oncology annual meeting], it was a little confusing because they had low platelets and thrombocytopenia, and I couldn’t quite figure out what the overlap was. That’s been clarified since then, and thrombocytopenia dropped from 38% to about 20%, which is pretty darn good. Most of us are using it; I use it if I see a patient like that. It starts at 200 mg rather than 300mg; you always have the option of going up if you want. There’s been some interesting mumbling in the background that maybe 200mg should have been the dose to begin with, but this is a perfectly reasonable compromise.
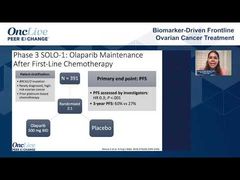
Bradley Monk, MD, FACOG, FACS: One of the interesting things is that the label for prescribing information of PRIMA is if the baseline weight is less than 77 kg, or if the baseline platelet count is less than 150,000, then you should start at 200mg, but it was not applied to the NOVA or QUADRA data. Although, to what Michael said, that’s what we’re going to do.
In the label, they show that there was no difference because you got to the right dose a cycle earlier. Patients sort themselves out based on toxicity in the first cycle, but that is impactful. At ASCO [the American Society of Clinical Oncology annual meeting], we’re not going to get into the specifics, but they even showed that, in the curves, there was no difference in the efficacy with the personalized dose.
Michael J. Birrer, MD, PhD: I’ll add, Brad, that it doesn’t mitigate the issue of getting weekly platelet counts when you put a patient on niraparib.
Bradley Monk, MD, FACOG, FACS: Thank you. We do that in my practice for all PARP inhibitors just to keep it simple. If the platelet count is less than 100,000, which would mean 99,999 or less, you should stop and reassess.
Transcript edited for clarity.
Advertisement
Related to this article

In case you missed any, check out our recap of the episodes of OncLive On Air that aired in June 2026.
Advertisement
Advertisement
Trending on OncLive
1
FDA Grants Fast Track Designation to Pelareorep in Pretreated SCAC
2
PRAME-Directed Therapies Advance Melanoma Treatment Across Clinical Settings
3
Dr Falchi on Critical Unmet Needs and Important Next Steps in DLBCL
4
Olverembatinib Plus Blinatumomab Yields High Early-Phase CR/CRi Rates in R/R Ph+ CML and B-ALL
5