
|Videos|February 1, 2018
The ExteNET Trial
Advertisement
Episodes in this series













Transcript:
Ruta D. Rao, MD: The ExteNET trial is a phase III double-blind randomized control trial. The patients enrolled in this trial had histologically confirmed stages 2 to 3c HER2-positive operable breast cancer. The original protocol involved patients with stages 1 to 3c, but this was later amended to be stage 2 to 3c. These patients had all received either neoadjuvant or adjuvant trastuzumab and completed up to 1 year of this. They were then randomized to neratinib or placebo, which was given continuously for 1 year following the completion of their adjuvant trastuzumab therapy.
The final analyses included the primary efficacy analysis of 2 years, which was done in July of 2014; the sensitivity analysis of the efficacy endpoints at 5 years, which was done in March of 2017; and the overall survival analysis, which is still pending 248 events.
The primary endpoint was 2-year invasive disease—free survival. This was defined as the time from randomization to the first occurrence of invasive ipsilateral tumor recurrence, invasive contralateral breast cancer recurrence, local or regional invasive recurrence, distant recurrence, or death from any cause.
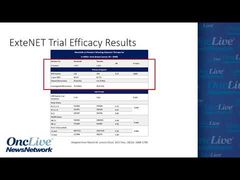
The trial enrolled 2840 patients and was reported with a median follow-up of 5.2 years. The invasive disease—free survival reported 116 events for the patients treated with neratinib versus 163 events for those treated with placebo. This resulted in a hazard ratio of 0.73 and a P value of .0083.
The 5-year invasive-free survival for neratinib was 90.2% versus placebo, which was 87.7%.
The invasive disease—free survival was then analyzed based on subgroups such as nodal status. The patients who were lymph node–negative had a hazard ratio of 0.83. There were 14 events in the neratinib-treated patients versus 19 in the placebo-treated patients. For those patients who had 1 to 3 positive lymph nodes, the hazard ratio was 0.75 based on 55 events in the neratinib-treated patients and 74 events in the placebo-treated patients. For those patients who had 4 or more positive lymph nodes, the hazard ratio was 0.67, based on 47 events in the neratinib-treated patients and 70 events in the patients who were treated with placebo.
Another subgroup that was looked at was based on hormone receptor status. For the hormone receptor—negative patients, the hazard ratio was 0.95. There were 57 events in the neratinib-treated patients and 63 in the placebo-treated patients. The hazard ratio was much more impressive for the hormone receptor–positive patients, with a hazard ratio of 0.60, resulting from 59 events in the neratinib-treated patients versus 100 events in the placebo-treated group.
You can see in the Kaplan-Meier curves from the publication in Lancet Oncology in 2017 the benefit of neratinib in the intend-to-treat population. There’s also a curve here separating the patients by their hormone receptor status, and you can see again that the hormone receptor—positive patients seem to have a benefit from neratinib, whereas the lines overlap for the patients with hormone receptor negativity.
Here you see the forest plots from the original publication, and you can see that essentially all subgroups did seem to favor neratinib over placebo. But when you specifically look at the subgroups we talked about, the node-positive patients seemed to gain a greater benefit, as do the hormone receptor—positive patients and those patients who started neratinib within a year of finishing their adjuvant trastuzumab.
When we analyze the adverse events seen in this trial, you can see that neratinib was associated with a significantly increased degree of diarrhea: 55% of patients who received neratinib had grade 1 to 2 diarrhea, and 40% had grade 3 diarrhea, compared with the placebo arm, in which 34% had grade 1 to 2 diarrhea and 2% had grade 3 diarrhea. Remember that this trial was done before they mandated the use of antidiarrheal agents. Other adverse events such as nausea, vomiting, abdominal pain, and rash were relatively equal between the 2 arms. There were slightly higher rates of grade 1 and 2 nausea, vomiting, abdominal pain, and rash for the patients who received neratinib versus placebo, but the rates of grade 3 or 4 incidence of these adverse events were equal between the 2 arms.
The CONTROL trial was an open-label study to characterize the incidence and severity of diarrhea in patients with early-stage HER2-positive breast cancer treated with neratinib and intensive loperamide prophylaxis. You can see from this table here that loperamide prophylaxis significantly reduces the incidence of diarrhea compared with the rates that were seen in ExteNET trial. The addition of budesonide, which is a long-acting corticosteroid, or colestipol, which is a bile-sequestering agent, to loperamide in these trials further improved the tolerability of neratinib by reducing the number and severity of diarrhea events. The final analysis of the CONTROL trial will be done after all patients have completed 12 months of therapy.
Transcript Edited for Clarity
Advertisement
Related to this article

Catch up on insights into the global development of breast cancer treatments in the global spotlight.

Dato-DXd was approved in the European Union as monotherapy for patients with first-line metastatic TNBC who are not candidates for immunotherapy.

The FDA issued final guidances on performance status, washout periods, and laboratory values aimed at expanding oncology trial participation.

The FDA accepted an NDA for daraxonrasib in metastatic pancreatic cancer, approved zidesamtinib in pretreated ROS1-positive NSCLC, and more.

The CHMP recommended EU approval of T-DXd plus pertuzumab as first-line therapy for HER2-positive metastatic breast cancer,

The CHMP has recommended the approval of sacituzumab govitecan/pembrolizumab for treatment-naive, PD-L1-positive metastatic TNBC in the European Union.

Watch a highlight reel of breast cancer data from ASCO 2026 that experts anticipate will have the biggest impact on the field.
Camizestrant plus a CDK4/6 inhibitor was approved in the European Union for ER-positive, HER2-negative advanced breast cancer with an emergent ESR1 mutation.
Advertisement
Advertisement
Trending on OncLive
1
FDA CTGTAC Votes in Favor of RP1/Nivolumab Data in Advanced Melanoma
2
FDA Grants Priority Review to Subcutaneous Amivantamab in Head and Neck Cancer
3
Dr Barot on the FDA Approval of Palbociclib/Trastuzumab ± Pertuzumab in HER2+ Breast Cancer
4
Dana-Farber Researchers Identify CDK8 as a Potential Therapeutic Target for Alveolar Rhabdomyosarcoma
5