
|Videos|July 20, 2020
Treating BRCA+ Ovarian Cancer
Advertisement
Episodes in this series















Bradley Monk, MD, FACOG, FACS: I want to talk about the HRP [homologous recombination proficient] subset in a minute. I don’t give up that easily though, Leslie; you know me.
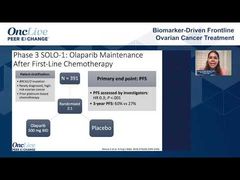
As you know, BRCA1 is more pathogenic; BRCA1 is more common in ovarian cancer. The risk of ovarian cancer is greater if you have a BRCA1 germline mutation, and BRCA1 is more difficult to treat with a PARP inhibitor. If you look at the BRCA1 and the BRCA2 efficacy data in SOLO-1, there’s slippage.
Leslie Randall, MD, FACOG: Right.
Bradley Monk, MD, FACOG, FACS: BRCA2 does better, but if you look in PRIMA, the BRCA1 patients do about as good as BRCA2. That supports Dr Birrer’s hypothesis that niraparib is a more potent PARP inhibitor because it works in the subset of BRCA1, BRCA2. I want your opinion and what you’re going to do in your practice.
Let’s say there’s a contraindication to bevacizumab, and let’s say your patient has a BRCA mutation, and you have the option, as per PRIMA, to use niraparib, or as per SOLO-1 to use olaparib. Both are NCCN [National Comprehensive Cancer Network] recommended, level 1. What are you going to do? BRCA1 mutation.
Leslie Randall, MD, FACOG: PARP inhibition alone is enough for BRCA mutated.
Bradley Monk, MD, FACOG, FACS: Which one? Olaparib or niraparib in the patient with a BRCA1 mutation? They’re both NCCN recommended. We’re going to get to that too; I don’t agree with you.
Leslie Randall, MD, FACOG: I’ve been using olaparib for almost 2 years.
Bradley Monk, MD, FACOG, FACS: On April 29th, the world pivoted. Some people say that you can now use the better PARP inhibitor in that patient with a BRCA mutation.
Leslie Randall, MD, FACOG: Yes. We’ve been having this discussion ever since platinum-sensitive recurrence, right? Which PARP inhibitor is better? We’ve had 3 indicated in the space, but still, what am I going to do? Should I just say my preference? I would use niraparib in that setting.
Bradley Monk, MD, FACOG, FACS: OK. I’m not going to hold the rest of everyone accountable, Leslie was my follow-up.
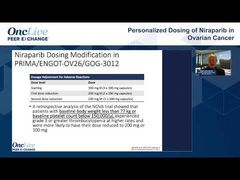
Leslie Randall, MD, FACOG: Do you want to know what I do in my practice? I choose for very practical reasons. I choose for a patient who can’t remember to take a drug twice a day. I choose for a patient who I need a lot of dose flexibility on. I don’t have that with niraparib because most of my patients are going to go down to 200 mg, or start at 200 mg, and then go to 100 mg, and then I’m done. If I need more dose flexibility, I’m going to be using olaparib.
Bradley Monk, MD, FACOG, FACS: To support you, as I always try to do, I would make the same decision, but because I like bevacizumab, I would want that patient to get bevacizumab-olaparib. I backed you into a corner.
Leslie Randall, MD, FACOG: I’m not in a corner because I haven’t decided that yet. I feel like the PARP inhibitor is enough, but if you look at the analysis presented at SGO [the Society of Gynecologic Oncology annual meeting], trying to pull in that olaparib-only arm that was not included in PAOLA; is olaparib alone enough? In that analysis, it showed that even the germline BRCAs benefit from the combination.
Bradley Monk, MD, FACOG, FACS: Give us the details of that paper, which did a weighted comparison. They could do it, right?
Leslie Randall, MD, FACOG: It has a very specific name, the analysis….
Bradley Monk, MD, FACOG, FACS: Go ahead, Matt, tell us about it.
Leslie Randall, MD, FACOG: Go ahead.
Matthew Powell, MD: This was a population adjusted, indirect comparison combining SOLO-1 patients with PAOLA patients, so you get a 4-arm trial if you look at it in a simple manner.
You get your carboplatin-Taxol [paclitaxel] by itself; you get your carboplatin-Taxol [paclitaxel] with a PARP inhibitor; you get your carboplatin-Taxol [paclitaxel] with bevacizumab; and then you get the combination. If you look across there, you see that 24-month PFS [progression-free survival] for the best group, which is the combination group, was 82%. If you look at the bottom, which is the carboplatin-Taxol [paclitaxel] alone, it was 36%. You can walk through this population and see the benefit and the contributions of each intervention. You’ll see that it looks like it’s at least additive giving these 2 targeted therapies to the backbone of carboplatin-paclitaxel. It compels you to think about the combination that bevacizumab is helping. So 82% progression free at 2 years, it’s staggering.
Bradley Monk, MD, FACOG, FACS: Leslie, if olaparib makes bevacizumab better in the non-BRCA patient, or at least the HRD [homologous recombination deficient], why wouldn’t it work in the BRCA patient? I’m really killing you today.
Leslie Randall, MD, FACOG: Olaparib alone may be enough. To add bevacizumab, you may not get much more benefit, and you definitely get more toxicity.
Bradley Monk, MD, FACOG, FACS: What do you think Shannon? For the patients with BRCA mutations: olaparib, niraparib, or the combination?
Shannon N. Westin, MD, MPH, FACOG: For me, I have to make the decision right from the beginning. The population that I feel is most at risk has stage IV and ascites. For those patients, I am going to give the bevacizumab and then continue it with the olaparib. To Leslie’s point, it’s hard to know. I wish we had a better way of selecting who needs that additional benefit. I thought the analysis presented was compelling, but I want to see the paper and all the details before I make some bold change. I do think there is a proportion of the patients with BRCA who are going to do just as well with the PARP inhibitor alone. If we can tease that out and understand it, it would be helpful.
Bradley Monk, MD, FACOG, FACS: BRCA patients do better, right? Michael, what do you think is the best treatment for BRCA1/2? What do you think about the bevacizumab combination?
Michael J. Birrer, MD, PhD: As you know, I give a lot of bevacizumab.
Bradley Monk, MD, FACOG, FACS: So do I; that’s what I just said.
Michael J. Birrer, MD, PhD: A lot of my patients are going to get a PARP inhibitor, olaparib, with bevacizumab. The interesting issue now that we’ve had multiple indications, and insurance companies are trying to wade through all this; it’s even conceivable to me that people are going to extrapolate from AVANOVA that niraparib may be combined with bevacizumab in some of these patients. I don’t necessarily think that’s wrong.
Bradley Monk, MD, FACOG, FACS: OVARIO. Go ahead, tell us about OVARIO.
Michael J. Birrer, MD, PhD: AVANOVA was in the recurrent setting combining niraparib with bevacizumab, showing it was safe and showing an advantage. Now that’s been moved up front with the trial that you mentioned, and I don’t think any of us will doubt that it’s going to be safe. It’s a single-arm, phase 2 study, so there’s only so much information that you’re going to get out of about 105 patients, somewhere in that range. But could I envision it showing good numbers, PFS, and safety, so leading to an expanded indication? It’s conceivable.
Bradley Monk, MD, FACOG, FACS: It was just presented at these meetings. Because it’s a single-arm trial, it probably won’t lead to FDA approval, but it might add to a compendium listing and create an opportunity.
Michael J. Birrer, MD, PhD: Correct. Let me say one other thing on this, Brad, because I know you’re thinking it, which is, all of these trials, combinations versus control arms, the 800 pound gorilla in the room that nobody looks at is sequencing.
Bradley Monk, MD, FACOG, FACS: That’s what I said, the NCI [National Cancer Institute] needs to do that.
Michael J. Birrer, MD, PhD: PAOLA-1 shows the combination is good. Can you get the same bang for your buck if you did it single-agent sequentially?
Bradley Monk, MD, FACOG, FACS: Right.
Michael J. Birrer, MD, PhD: We don’t know, and that’s the question that NCI should ask, right?
Bradley Monk, MD, FACOG, FACS: That’s Dr Randall’s point. Leslie’s point is can we get them to do it in sequence?
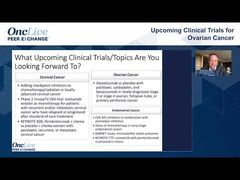
Leslie Randall, MD, FACOG: Here’s the problem with sequence that I’ve thought about. I’ve had to iterate these trials over in my head many, many times to come up with some of these thoughts. One thought is that, right now, your PARP inhibitor in the recurrent setting has restricted benefits to the platinum-sensitive population. Especially if you have an HRP patient who is likely to be platinum-resistant, front line may be your only opportunity to give them the PARP inhibitor. You may not have the option of sequencing PARP inhibitors until we get better combinations, which we’ll talk about later. Right now, single-agent PARP inhibitors are best given in the front line.
Transcript edited for clarity.
Advertisement
Related to this article

In case you missed any, check out our recap of the episodes of OncLive On Air that aired in June 2026.
Advertisement
Advertisement
Trending on OncLive
1
FDA Grants Fast Track Designation to Pelareorep in Pretreated SCAC
2
PRAME-Directed Therapies Advance Melanoma Treatment Across Clinical Settings
3
Dr Falchi on Critical Unmet Needs and Important Next Steps in DLBCL
4
Olverembatinib Plus Blinatumomab Yields High Early-Phase CR/CRi Rates in R/R Ph+ CML and B-ALL
5