
|Videos|February 1, 2021
Regorafenib in Third or Fourth Line for mCRC: Efficacy in the Re-DOS Trial
John Marshall, MD, reviews efficacy data from the ReDOS study of regorafenib in patients with mCRC.
Advertisement
Episodes in this series







John Marshall, MD: Let’s discuss Tony Bekaii-Saab, MD’s, trial to try to solve this. Because if you’re rapidly declining and you start somebody at 160 mg of regorafenib, it’s not going to work. They’re going to have bad hand-foot syndrome, they’re going to be tired, they’re going to be unhappy, and they’re going to request being removed from the trial and the treatment because they’re unhappy.
Axel Grothey, MD: And early on. Within a week, patients have these hand-foot skin reactions; they feel fatigued. You turn a patient who you think has good performance status and is a candidate for it, into a sick patient, if you use the old dosing strategy.
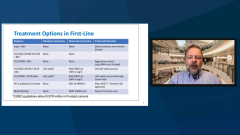
John Marshall, MD: The blogs, the advocacy blogs and everything started talking about don’t take that drug sort of thing. The lesson we learn, and Tony made it real, if you will, is that you need to know how to dose the medicine. As everybody knows, it’s typically 160 mg daily, 3 weeks on, 1 week off. As Axel was saying, most people get fairly significant adverse effects even within a week or two, unlike what we’re used to seeing with other drugs. People coming in, torn up hands and feet, and poor liver function.
Tony cleverly studied what we were all playing with and did it in a more formal way of looking at an escalating dose. Instead of starting at 160 mg, start at 2 pills at 80 mg, but for an entire week. Then see the patient again, as part of this study, and if they were fine and their laboratory tests were fine, then go up to 120 mg. Then if they were again fine one week later for week 3 of cycle 1, go up to 160 mg. If they tolerated that, then that was their starting dose for the next cycle. And if they didn’t, you went to the 120 mg, or whichever dose was the right one. And it was a smaller trial. It was also looking at some hand creams to try to prevent some of the skin reactions.
But the primary answer here was that if you started low and you went up, the primary end point was how many people made it into cycle 3. What you saw was that a lot more did. Not quite double, but nearly double made stable disease beyond the first 2 cycles. That’s basically what your trial, Axel, showed, and a lot of what I tell patients is that about half of everybody who takes regorafenib has stable disease or better at the first scan, which is at 8 weeks or so. That was borne out because about half of these people made it into cycle 3, just under half.
By dosing it this way you were able to avoid that early stop, the patient who gave up on their treatment, and then therefore didn’t find out whether they benefitted.
Then of course we have the OS [overall survival]. Now remember the previous slide I showed you was statistically significant with a good hazard ratio. This one not because it wasn’t powered for overall survival, but you clearly get a trend. It wasn’t worse, and we can say that even with a nonstatistical trial of this size. Whether we believe it’s better or not, you can think that if you like, but it trended that way. Again, small numbers but certainly suggesting that dosing this way, which is more labor intensive, I don’t want anybody to forget that. It requires monitoring by either a nurse practitioner or a physician.
We’re working on an app where we load it on the patient’s phone, and each day they tell us how many pills they’re talking. We list 5 toxicities. If it gets to a certain level, it sends a note to one of us so we can whether they’ve gotten their labs, that sort of thing.
I do think technology is making this easier, but it’s not a, “Send them a prescription, I’ll see you in a month,” kind of prescription. You must watch them more closely.
Transcript Edited for Clarity
Advertisement
Related Content


































































Advertisement
Advertisement
Trending on OncLive
1
FDA Grants Priority Review to Giredestrant for ER-Positive Early Breast Cancer
2
Breast Cancer Experts Spotlight Practice-Informing and Thought-Provoking Data From ASCO 2026
3
Bispecific-Based Approaches Highlight Key Multiple Myeloma Data Set to Emerge at EHA 2026
4
CELMoDs and Bispecifics Break Through Across Lymphomas and Leukemias at EHA 2026
5