
|Videos|November 9, 2022
Immunotherapy and You: The 5 Cs in Gynecologic Cancer
Author(s)John Nakayama, MD, Ali Amjad, MD
In this third episode of OncChats: Immunotherapy and You, John Nakayama, MD, and Ali Amjad, MD, review the 5 C's to consider when conducting research in gynecologic cancers and beyond.
Advertisement
Episodes in this series

In this third episode of OncChats: Immunotherapy and You, John Nakayama, MD, of the Division of Gynecologic Oncology, Allegheny Health Network, and assistant professor of OBGYN at Drexel University, and Ali Amjad, MD, medical hematologic oncologist, Allegheny Health Network, review the 5 C's to consider when conducting research in gynecologic cancers and beyond.
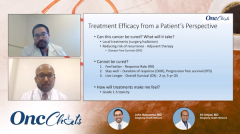
Nakayama: When we were talking earlier, you came up with these 5 C's of cancer research. Could you explain to our audience what you mean by that?
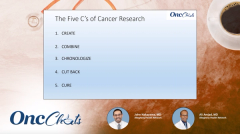
Amjad: Yeah, so this is something that I think about a lot. Being in medical oncology, we have to have a framework of how research develops and how our treatment paradigms are created. [To this end,] I have this 5 'C' model of cancer research.
The [first] 'C' [stands for] create. Many times, we have to have a new discovery. In the context of immunotherapy, we have created 7 to 8 checkpoint inhibitors. Once we have an effective therapy, we always try to combine it with other therapies to see whether the efficacy can be improved. We have plenty of examples where immunotherapy can be combined with either chemotherapy, other immunotherapy agents, TKIs, [and other agents]. Those combinations, many times, do work better than just the single agents.
Once we have an effective single agent or a combination, we try to chronologize or sequence them in a way that we can improve efficacy. Many of these cancer treatments are developed in the advanced-stage setting—third-line, fourth-line treatments—and then they get moved to an up-front setting [for analysis]. Like we discussed before, immunotherapy is now being utilized in the adjuvant setting to improve disease-free survival, [for example]. Then, we have effective therapies, we to see if we can cut back on them to see whether we can [still achieve] a similar effect. We [see if we] can identify biomarkers that can select a population [for whom] we can just [give] less than the traditional treatment. For example, if we use chemoimmunotherapy in lung cancer, how about if we use a biomarker to select a population that will do equally good or even better with immunotherapy alone? That is always the goal for us: to do less and get more. Obviously, as doctors and researchers, we want to cure our patients.
So that seems to be my 5 'Cs,' a simplistic way for thinking about cancer care.
Check back next Wednesday to view the next segment in this series.
Advertisement
Related to this article

First-line pembrolizumab monotherapy met the primary end point of PFS in dMMR advanced/recurrent endometrial cancer.

The phase 3 OptiTROP-Lung06 trial showed a PFS improvement with sac-TMT plus pembrolizumab in PD-L1–negative NSCLC.
Advertisement
Advertisement
Trending on OncLive
1
FDA Grants Fast Track Designation to Pelareorep in Pretreated SCAC
2
PRAME-Directed Therapies Advance Melanoma Treatment Across Clinical Settings
3
Dr Falchi on Critical Unmet Needs and Important Next Steps in DLBCL
4
Olverembatinib Plus Blinatumomab Yields High Early-Phase CR/CRi Rates in R/R Ph+ CML and B-ALL
5