
|Videos|September 20, 2021
Case 5: A 24-Year-Old Female With Well-Differentiated SM
Sa Wang, MD, presents the case of a 24-year-old female with well-differentiated systemic mastocytosis.
Advertisement
Episodes in this series






Sa Wang, MD: I want to move to the second case. I think it’s a very good contrasting case to show you. This is a 24-year-old woman. The patient had a lot of skin lesions since childhood. I think the age, it really went back to when she was a couple of years old. It is urticaria pigmentosa. All the way, tracing this patient’s history, we actually published this case, all the symptoms started when she was 4 years old, with all the skin lesions. Then, when she was 17 years old, she started to have a lot of GI [gastrointestinal] symptoms and also there were systemic symptoms with joint pain and weight loss. When she was 24 years old and she was diagnosed with gastric mastocytoma, it was 4.3 cm in the largest dimension. That was the time when the patient came to us and did a bone marrow biopsy. If you see this bone marrow…mast cells. Similar to last case, these cells are very round instead of spindly, but they do form aggregates. I would not say they’re tight clusters, but they are loose clusters. Some of the mast cells even look like they have intrusion, but they do have lots and lots of granules. I want to show you this from my aspirate smear. You can see they have so many granules. It’s very hard to photograph them because they are so dark. This is the background…cells.
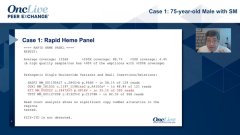
Another thing about this artificial 20% cutoff, we always say when the cells aggregate, where you cannot see, you should not count, but you can see a lot of mast cells actually in this area, they are in aggregates. This will also be more than 20%, but these cells are very well differentiated. They almost look like the normal mast cells and have lots and lots of granules. They are roundish in shape. Then, we did a flow cytometry. These cells actually did not have CD2, and they also did not have CD25. However, they do have CD30. Concerning aberrant markers, we always talk about CD2 and CD25; actually, CD20 is another marker. This was an aberrant expression of about 80% SM [systemic mastocytosis]. In the past, they saw it only in aggressive SM, but that’s not true. When we did the study and also captured by the Spanish group, they show 80% cells actually aberrant express CD30. We also confirmed this in the immunohistochemistry, we can see the mast cells very uniformly pass for CD30. The patient’s tryptase was elevated, and KIT D816V by high-sensitivity PCR [polymerase chain reaction] was also negative. Also, FISH [fluorescence in situ hybridization] for PDGFRA was negative, normal karyotype. But then, when we did NGS [next-generation sequencing], we found that the patient had a canonical KIT mutation. This diagnosis was a well-differentiated SM. Some may call this chronic mast cell leukemia because there are more than 20% mast cells on the bone marrow aspirate smear, but we know that this is well-differentiated SM.
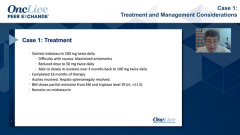
What is unique about this type of SM? The patient usually has skin involvement, they are really round shaped. They are largely CD25 negative. Of course, CD2 will be negative, and they do have elevated serum tryptase. They usually lack the typical KIT D816V mutation. However, they do have aberrant expression of CD30. If we see here, 8 out of 9 cases actually express CD30, and none of them express CD25. So CD30 can help to identify aberrancy in the cells because when we have this type of SM the question is, is this reactive mast cell hyperplasia, or is it actually a systemic mastocytosis because they so much look like normal mast cells? CD30 can help you to identify this is as an aberrant mast cell. Also, when we review the literature, it’s interesting, the reported cases, several of them have a noncanonical KIT mutation, not an D816V, in other loci within the KIT, and also these patients actually responded beautifully to the TKI, or tyrosine kinase inhibitor. To identify this mutation is very important. Our patient actually responded beautifully to TKI, and all the symptoms resolved, skin lesions, and systemic symptoms. However, actually, she was noncompliant, and it came back, she recurred again with SM.
I just wanted to illustrate that this is a case where it can be confused with mast cell leukemia. Or you can call this chronic mast cell leukemia because they are really not aggressive, this disease. Also, if you identify this morphology and look for this KIT mutation in the D816V region, you can find the patient can respond to TKI therapy.
Transcript edited for clarity.
Advertisement
Related to this article

The top 5 OncLive TV videos of the week cover insights in breast cancer, uveal melanoma, colorectal cancer, multiple myeloma, and sarcoma.

The FDA approved Orca-T, issued a CRL to a NET imaging agent, and more.

Divesiran lowered phlebotomy needs, raised ferritin, and improved MPN-10 symptom scores in phlebotomy-dependent polycythemia vera.

A Dana-Farber study identified an RNA surveillance defect that fuels melanoma through endogenous retroviral RNA.

Belantamab mafodotin–based therapy improved sustained MRD negativity rates in relapsed/refractory multiple myeloma.

Updated COMMANDS data showed durable RBC transfusion independence and a positive overall survival trend with luspatercept in lower-risk MDS.

Robert A. Winn, MD, discussed his path to becoming a physician, scientist, and leader at Fox Chase Cancer Center.

Updated analyses from a phase 2a study suggest durable survival with namodenosen in a subset of heavily pretreated patients with advanced PDAC.
Advertisement
Advertisement
Trending on OncLive
1
Managing Long-Term Toxicities and Emerging Therapies in ALK-Positive NSCLC
2
Five Under 5: Top Oncology Videos for the Week of 6/28
3
The OncFive: Top Oncology Articles for the Week of 6/28
4
Divesiran Reduces Phlebotomy Burden and Improves Iron Stores in Polycythemia Vera
5