
|Videos|September 27, 2021
Case 6: 47-Year-Old Male With Leukocytosis, Anemia, and Splenomegaly
Sa Wang, MD, presents the case of a 47-year-old male with leukocytosis, anemia, and splenomegaly.
Advertisement
Episodes in this series






Sa Wang, MD: I’m moving on to the last case. This 47-year-old patient presents with leukocytosis, anemia, splenomegaly. WBC [white blood cell count] was 57,000. It was 21% monocytes, anemic, and platelets were actually elevated. This is the bone marrow biopsy. We do have a little bit of thickening of the bone, but what you notice in this part is there are a lot of megakaryocytes; on the higher part you see megakaryocytes are very small and dysplastic. These are megakaryocytes, so we know we are dealing with very hypercellular, with dysplastic karyocytes. This patient with monocytosis, immediately we’re thinking, could this be CMML [chronic myelomonocytic leukemia]? Another thing you notice is that we do have a slight increase in eosinophils in this patient. But here, in some areas it looks like there are a little bit of spindle cells. However, when you have a diagnosis, you say, “Wow, I already got my diagnosis of CMML.” Then, CMML can have liver fibrosis. It’s nothing surprising. In this case, you can see here on the bone marrow aspirate smear, we have blasts. We have myeloid precursor monocytes. When we did the CD34, the patient does have CD34 clustering, which further supports the diagnosis of myeloid neoplasm, and also CD34 was about 5%. The diagnosis was CMML. We actually did flow cytometry. You see the CD34 cells, they had aberrancy of CD56 expression, have the aberrant CD5 expression, and also aberrant CD34 and CD117. The monocytes were 15.2%. Everything goes very well with CMML, so the diagnosis was CMML.
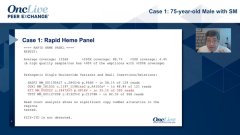
About 70% of patients with CMML have a normal karyotype, but the NGS [next-generation sequencing] came back, and we had a KIT mutation and ASXL1 and U2AF1. The KIT mutation burden was very high at 41%. We actually went back to look for the mast cells in this case. When we did CD117, you can see the mast cells were very focal. I amplified this, with the higher power you do see the cells, the spindle cells, but it was completely ignored. No one can blame anyone for missing these small mast cell aggregates. You can see, as I said, when you see a mast cell in the future, in the surrounding, you see some eosinophils on the edge. It’s very common to see mast cells. The rest of the mast cells are very scattered, few spindles, but that is the whole bone marrow biopsy. We only have this little bit of mast cell aggregate. I go back to this, according to Dr…you’re supposed to call this SM [systemic mastocytosis], associated with hematologic malignancy with underlying disease and CMML. However, we all know this is probably a dominant disease, it’s a chronic myelomonocytic leukemia with very focal mast cell. Proliferation or differentiation, both are quite clear of SM. With SM, you have more than 15 cells in aggregate, and they are mostly spindly, and also you have KIT mutation with…criteria. We also had flow cytometry, this is when the patient came back…you can see they are CD30 positive, CD25 positive, and no CD2.
I think this case raises a number of questions. This is apparently KIT-mutated myeloid neoplasm. Is the presence of the small mast cell aggregate relevant in this case? If we call this according to the WHO [World Health Organization] criteria, how do you assess the C findings because underlying neoplasm in CMML can cause the anemia? Another question is, concerning this patient, are they going to respond to this mast cell inhibitor like avapritinib? In this case, if the mast cell infiltrate is more than 30%, how is that going to change your assessment and management? I think this question, as a pathologist, I raise for you the clinicians.
Transcript edited for clarity.
Advertisement
Related to this article

The top 5 OncLive TV videos of the week cover insights in breast cancer, uveal melanoma, colorectal cancer, multiple myeloma, and sarcoma.

The FDA approved Orca-T, issued a CRL to a NET imaging agent, and more.

Divesiran lowered phlebotomy needs, raised ferritin, and improved MPN-10 symptom scores in phlebotomy-dependent polycythemia vera.

A Dana-Farber study identified an RNA surveillance defect that fuels melanoma through endogenous retroviral RNA.

Belantamab mafodotin–based therapy improved sustained MRD negativity rates in relapsed/refractory multiple myeloma.

Updated COMMANDS data showed durable RBC transfusion independence and a positive overall survival trend with luspatercept in lower-risk MDS.

Robert A. Winn, MD, discussed his path to becoming a physician, scientist, and leader at Fox Chase Cancer Center.

Updated analyses from a phase 2a study suggest durable survival with namodenosen in a subset of heavily pretreated patients with advanced PDAC.
Advertisement
Advertisement
Trending on OncLive
1
Managing Long-Term Toxicities and Emerging Therapies in ALK-Positive NSCLC
2
Five Under 5: Top Oncology Videos for the Week of 6/28
3
The OncFive: Top Oncology Articles for the Week of 6/28
4
Divesiran Reduces Phlebotomy Burden and Improves Iron Stores in Polycythemia Vera
5