
|Videos|September 20, 2021
Well-Differentiated Systemic Mastocytosis vs Chronic Mast Cell Leukemia
The panel of experts discuss the clinical differences between well-differentiated systemic mastocytosis and chronic mast cell leukemia.
Advertisement
Episodes in this series






Dan DeAngelo, MD, PhD: That’s a phenomenal presentation of a very a rare disease. Now, we’re talking about hen’s teeth in a rare disease. I have seen a lot of mast cells, but I have only seen 2 cases of well-differentiated systemic mastocytosis [WDMS], and both were misdiagnosed at the outside center. One of my patients was more of an indolent finding, as you mentioned, these can be very indolent. However, the other case presented with mastocytoma, and she responded well to imatinib. How many cases are you seeing, Dr Wang, for these?
Sa Wang, MD: Not many, but recently we saw another case. We actually have a fellow who just brought it up. It’s another case. We do see it once in a while. I think the important thing is not to say this is mast cell hyperplasia because mast cell hyperplasia sometimes can be associated with a lot of conditions like lymphoplasmacytic lymphoma, and they can have lot of mast cells. Just don’t get confused with that.
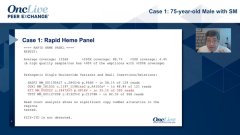
Dan DeAngelo, MD, PhD: I think the important thing here is that the D816V is almost, at least in my understanding, ubiquitously wild type, you don’t see the D816V. And the digital droplet PCR [polymerase chain reaction] is really specific for that, so it’s important to do really a full KIT mutation because you find mutations that are outside of the pseudo activation center within D816V. They are elsewhere within the juxtamembrane, or other components of the gene, so the whole gene really needs to be sequenced, and you can see the different mutations that you’re showing here on these cases.
Sa Wang, MD: A patient who did NGS [next-generation sequencing] would identify this mutation.
Dan DeAngelo, MD, PhD: Dr Bose or Dr Lugar, any thoughts on this rare entity?
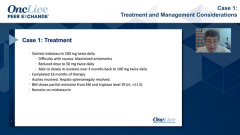
Prithviraj Bose, MD: I haven’t seen WDSM myself. But, of course, I am aware of it, and it’s a great reminder of where imatinib can help. As you said, Dan, it can encompass the entire spectrum of indolent to smoldering to advanced. Speaking of CD30, we had done the trial of brentuximab vedotin, the antibody-drug conjugate, with Jason Gotlib, MD. That unfortunately was disappointing. So far, that approach has not worked.
Sa Wang, MD: That’s correct. I remember many years ago I implemented CD30 to our flow panel. It’s because of that trial. However, we found it was actually very useful for us for diagnostic purpose.
Transcript edited for clarity.
Advertisement
Related to this article

Lyudmila Bazhenova, MD, FASCO, outlines key considerations for treatment intensification in EGFR-mutated NSCLC.

Five Huntsman Cancer Institute at the University of Utah colleagues earned endowed chair appointments, including new appointments.

The CHMP recommended EU approval of T-DXd plus pertuzumab as first-line therapy for HER2-positive metastatic breast cancer,

Did you catch all of this week's top oncology news? Test your knowledge with OncLive's Weekly News Quiz.

The CHMP has recommended the approval of sacituzumab govitecan/pembrolizumab for treatment-naive, PD-L1-positive metastatic TNBC in the European Union.

Overall survival was the sole US primary end point of the phase 3 EPCORE DLBCL-1 trial evaluating epcoritamab and was not met.

Watch a highlight reel of breast cancer data from ASCO 2026 that experts anticipate will have the biggest impact on the field.

Teclistamab plus talquetamab met the primary PFS end point and improved overall survival in relapsed/refractory multiple myeloma in MonumenTAL-6.
Advertisement
Advertisement
Trending on OncLive
1
Dr Pant on the Potential Significance of Daraxonrasib for PDAC Management
2
Breast Cancer Buzz at ASCO 2026: De-Escalation Strategies, Targeted Therapies, and More
3
Epcoritamab Misses Sole US Primary End Point of Overall Survival in R/R DLBCL
4
Dr Lee on the Optimal Duration of Adjuvant Osimertinib in EGFR+ NSCLC
5