
|Videos|September 7, 2021
Case 3: Indolent Systemic Mastocytosis
Dan DeAngelo, MD, PhD, presents the case of a patient with indolent systemic mastocytosis and urticaria pigmentosa.
Advertisement
Episodes in this series

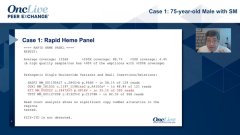





Dan DeAngelo, MD, PhD: I think the next case will be right up your alley, Dr. Lugar, in terms of highlighting a case that was a challenge. This is a patient of mine who presented with urticaria pigmentosa, 15 years ago now, 2006; and more prominent symptoms, hive-like symptoms, with heat or after hot water exposure. She had an isolated episode of syncope. She had a tryptase of just about under 80, and a skin biopsy. It’s representative of what she has. She just has spots everywhere. A skin biopsy confirmed urticaria pigmentosa, or cutaneous mastocytosis. Given her tryptase level, she was referred to hematology for a bone marrow exam. That showed about 10% dense aggregates, consistent with systemic mastocytosis. She had a KIT D816V mutation. She had no other mutations, isolated. I’m not going to show you her bone marrow, for brevity, but she had normal counts and no C-findings. She was diagnosed as having indolent systemic mastocytosis and was managed by allergy and immunology with respect to her symptoms with a cocktail; with H1 and H2 blockers and montelukast [Singulair].
She did well. She’s a fourth-grade schoolteacher, and she did well. She developed a cough. She’s a nonsmoker. Sure enough, she had a mass that was biopsied, and she has non-small cell lung cancer with an EGFR mutation and was started on erlotinib [Tarceva]. She did great for 3 years when she developed small brain metastases, unfortunately. They tried to make the switch to Osimertinib [Tagrisso], and she anaphylaxed, so they switched her back to erlotinib. Allergy/immunology has been on board all around. They do a desensitization program. I’m not exactly sure what that means. Maybe you can tell us.She has recurrent anaphylaxis, so she goes back to erlotinib, and she has some slight progression.
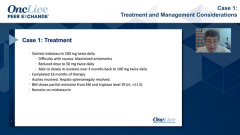
They tried desensitization in the ICU [intensive care unit] again, and she anaphylaxes yet again, so they’re stuck. Of course, I get paged, and I get called. She doesn’t meet the criteria, so with all due diligence, this is a non-FDA [Food and Drug Administration] approved indication for midostaurin [Rydapt]. She does have systemic mastocytosis, but she has no C-findings, so it’s indolent. But I didn’t know what else to do, so I started her on midostaurin, 100 milligrams, twice daily. I drove down her tryptase, and I’ll show you in the next slide. We were able to start osimertinib at 40 milligrams. I started her in the hospital because I was afraid. She had no reaction. And after a month, I increased the dose to 80 milligrams, and all of her lesions resolved. And this is her tryptase showing a rise to 140 about, and then on the midostaurin, really dropping precipitously to around 20, which is where it is today. There’s a little blip when we went down on the dose of the midostaurin because she was having some GI [gastrointestinal] toxicity. Then, she re-escalated. She had just these very subtle ditzels in her brain that are now really resolved.
She had an MRI [magnetic resonance imaging] just recently, May 2021, showing resolution. Not to highlight the point here, but this is just the cutaneous involvement that I pulled off. This is not her, but somebody else, just showing, again, the H&E [hematoxylin and eosin stain] on the left and the amount of tryptase-positive mast cells. This is a CD25 stain, however, on the right, just highlighting the amount of involvement. This is a flow diagram, which is what we do here, in addition to the IHC [immunohistochemistry staining]. I’m not sure we really need it. But here, you can identify, in the right upper outer quadrant, patients that are CD2, CD117, and CD25-positive cells, which really meets all the criteria. CD117 is ubiquitously expressed, and CD25 and CD2 are often—the one caveat to that is, often, treatment with avapritinib [Ayvakit] or midostaurin will down-regulate the CD25, so it can be hard to follow later. With that, I’m going to stop sharing. Dr. Lugar, thoughts?
Patricia Lugar, MD, MS: You did a fantastic job, Dan, I have to say.
Dan DeAngelo, MD, PhD: Who would’ve thought?
Patricia Lugar, MD, MS: I would have done the same thing. Desensitization in mastocytosis is certainly not as successful as somebody without mastocytosis. I had mentioned we sometimes use omalizumab [Xolair], and that’s actually what I thought you were going to say next, but you were even more brilliant because you went ahead and just treated it. I think that’s exactly what you have to do. It makes complete sense that she would’ve responded then with the reduction in mast cell burden. Your only options are to do anything you can to reset that reactivity of the mast cells. You are not going to get around it any other way. We’ve tried desensitization again, and again, and again in these patients that are hospitalized, and it’s very difficult to be successful. It just is. We’re lucky we can do that with venom anaphylaxis. They do respond to allergen immunotherapy. But drug desensitizations are very, very difficult. We just don’t have a lot of success in that venue, so you’re really looking for any other options to mitigate the disease.
Dan DeAngelo, MD, PhD: Dr. Bose?
Prithviraj Bose, MD: This is a brilliant case. I mean, the midostaurin clearly enabled her to receive a lifesaving or life-prolonging therapy. That right there, it’s a huge deal. And avapritinib, too. Bruce Bochner has published a case where there was recurrent anaphylaxis that was successfully treated with avapritinib, so I guess we’re going to perhaps see more of this use of these drugs.
Dan DeAngelo, MD, PhD: It’s off label, so for all due diligence, I did say that. But I think when these patients are pushed up against a wall, we really have no option. Sometimes, you have to think outside the box. If the disease is causing the anaphylaxis, treating the disease will help. And we were lucky, and she’s still doing well. Those slides were updated just a month ago.
Transcript edited for clarity.
Advertisement
Related to this article

The top 5 OncLive TV videos of the week cover insights in bladder cancer, chronic myeloid leukemia, multiple myeloma, pancreatic cancer, and chronic lymphocytic leukemia.

The FDA approved gedatolisib in PIK3CA wild-type breast cancer, granted full approval to selpercatinib in RET fusion+ tumors, and more.

Two optimized CD33-directed CAR T-cell therapies generated complete remissions with incomplete count recovery in heavily pretreated relapsed/refractory AML.

Lung cancer experts discuss the optimal management of CNS disease in EGFR-mutated non–small cell lung cancer.

Data for fixed-duration regimens in CLL suggest benefits over chemoimmunotherapy but still require improvements for high-risk patients.

Laure-Anne Teuwen, MD, PhD, debates the real-world advantages of subcutaneous pembrolizumab.

Iza-bren was approved in China for recurrent or metastatic ESCC following progression on platinum-based chemotherapy and PD-1/PD-L1 inhibition.

A research team from Huntsman Cancer Institute at the University of Utah showed a pathway-targeted therapy that could be an effective melanoma treatment.
Advertisement
Advertisement
Trending on OncLive
1
Frontline Sac-TMT Plus Pembrolizumab Meets PFS End Point in PD-L1–Negative, Nonsquamous NSCLC
2
The OncFive: Top Oncology Articles for the Week of 7/12
3
Five Under 5: Top Oncology Videos for the Week of 7/12
4
CD33-Directed CAR T-Cell Therapies Elicit Complete Remissions in Relapsed/Refractory AML
5