
|Videos|September 13, 2021
Case 4: Treatment and Management Considerations in MCL
The panel of experts in SM discuss the diagnosis and treatment of a 68-year-old female with mast cell leukemia.
Advertisement
Episodes in this series






Sa Wang, MD: I don’t know if anyone wants to make any comments about a mast cell leukemia [MCL] diagnosis. First of all, do you think the only requirement being more than 20% mast cells on an aspirate smear is a good criterion, or that this is just 1 form of aggressive systemic mastocytosis [SM]?
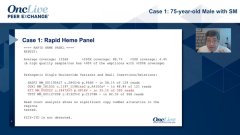
Dan DeAngelo, MD, PhD: You raise an excellent point as this is an artificial thing, so it’s an aleukemic leukemia, if you will. There is no circulating or very minimal circulating disease, and the mast cells are just really on that bone marrow aspirate. Then, you’re subjugate to the quality of the aspirate because some aspirates are more cellular than others due to the fibrosis. There must be something different about it. In my one hat, I think this is an artificial diagnosis; in the other hat, study after study after study even with these patients with aleukemic leukemia, they seem to have a lower response rate, and you’ve already mentioned that the KIT mutation and CD25 frequency is a little bit different. There is something different about these patients and the ability to have these aspirate smears with 20%, although is 19% really any different than 20%, but 20% is the bar in the sand. Dr Bose?
Prithviraj Bose, MD: You know Dan, I think the main thing here regarding what needs to guide us is what is the survival, what’s the natural history? I think if we go back to the old Mayo Clinic paper as well as the more recent ECNM [European Competence Network on Mastocytosis] paper, they are doing worse generally than ASM [aggressive systemic mastocytosis] and SM-AHN [SM with associated hematologic neoplasm] and I think that is what needs to really set this apart. However, we know about the chronic MCL, which is a variant that seems to behave a lot less aggressively and is not associated with C findings. Clearly, it’s a heterogeneous group.
Sa Wang, MD: Definitely, I think you’re right concerning this point, which is why we’re looking into this mast cell leukemia…cases from MD Anderson Cancer Center. Some are very aggressive, whereas some are very indolent. Actually, that’s why when the people who created these entities realized that some are not aggressive, they then created this chronic mast cell leukemia entity. I think it has a lot to do with the cytology of the cells. They are very roundish, they’re anaplastic. They look much higher grade, and also the underlying molecular genetic findings of this disease. Probably, those dictate the artificial cutoff of 20%.
Transcript edited for clarity.
Advertisement
Related to this article

Teclistamab plus talquetamab met the primary PFS end point and improved overall survival in relapsed/refractory multiple myeloma in MonumenTAL-6.

The FDA has granted priority review to a supplemental application for talazoparib plus enzalutamide in HRR-altered mCSPC.

Camizestrant plus a CDK4/6 inhibitor was approved in the European Union for ER-positive, HER2-negative advanced breast cancer with an emergent ESR1 mutation.
The FDA is reviewing data for daraxonrasib in previously treated pancreatic cancer under the Commissioner’s National Priority Voucher program.

Johannes Schetelig, MD, MSc, discusses phase 3 data for post-transplant cyclophosphamide vs ATLG as GVHD prophylaxis in hematologic malignancies.

Matthew Galsky, MD, discusses the FDA approval of perioperative pembrolizumab plus enfortumab vedotin in MIBC.

The FDA has approved zidesamtinib in patients with locally advanced/metastatic ROS1+ NSCLC who received a prior ROS1 kinase inhibitor.

A 3-year, $225K award will focus on improving quality of life for patients living with long-term effects of cancer treatment.
Advertisement
Advertisement
Trending on OncLive
1
FDA Accepts NDA for Daraxonrasib in Previously Treated Metastatic Pancreatic Cancer
2
FDA Approves Zidesamtinib in Pretreated ROS1+ NSCLC
3
Dr Patel on the Unmet Need in EGFR+ Transformed Small Cell Lung Cancer
4
Dr Galsky on Systemic Therapy Advances in Muscle-Invasive Bladder Cancer
5