
|Videos|August 2, 2021
Considerations in Mast Cell Disorders
The panel of experts highlights the importance of assessing symptomology and clinical characteristics in mast cell disorders.
Advertisement
Episodes in this series






Dan DeAngelo, MD, PhD: It’s an important point. I’ve seen a lot of referrals, and I’d like to get your opinion, Dr Bose, in terms of where patients have had outside GI [gastrointestinal] biopsies or liver biopsies and the referral had no mast cell involvement. The special stains weren’t done, and these diagnoses can be missed. We looked at our database at Brigham and Women’s Hospital and Dana-Farber Cancer Center—the patients we had in NGS [next-generation sequencing] KIT mutation, D816V, went back and looked at the pathology, and we’re able to identify about a third more cases. Is this something people should be concerned about? Prithviraj?
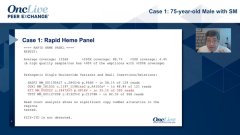
Prithviraj Bose, MD: You’re exactly right, especially if it’s a GI or some other nonheme presentation and SM [systemic mastocytosis] is not on the radar, then absolutely it could be missed. Also, what you just said reminded me of the limitations of the NGS panel, so we may miss KIT mutations. Three years ago, we started doing the digital droplet PCR [polymerase chain reaction] here to pick up the KIT D816V. Actually, I had a patient on PATHFINDER who had only GI involvement and no marrow involvement.
Dan DeAngelo, MD, PhD: Interesting. To throw the baton to you, Dr Lugar, there are two questions that we’re always struggling with. I’ll ask you, when is the appropriate care for patients with mast cell activation syndrome? Some patients with mast cell activation syndrome clearly have systemic mastocytosis, but others don’t. How are you making the diagnosis of this disorder? What’s your approach in terms of treatment? I have 1 follow-up question after that.
Patricia Lugar, MD, MS: Thanks, Dan. That’s often a difficult clinical scenario to work through. You want to make sure that you have the correct diagnosis, but the symptoms certainly mimic many other symptoms that are cardiovascular or have origins in other organ systems; pulmonary; POTTS, or postural orthostatic tachycardia syndrome; and multiple food sensitivities and food allergies. The most important thing is, No. 1, how much do I believe the person has a mast cell disorder? Many patients will come to us with the diagnosis because they have spoken to friends or colleagues at work who have had that diagnosis or have looked on the internet and gotten some information, and they feel like their symptoms might fit a mast cell disorder. It’s quite challenging because, by symptomatology alone, it’s a very confusing space to figure out what the patient is experiencing. And we don’t have a number of fantastic clinical markers or biomarkers to also guide us for mast cell activation, as opposed to a true clonal mast cell disorder.
That’s where I begin, trying to tease out the symptoms, what brings on the symptoms, and what has worked. Then, from a clinical laboratory evaluation, I will measure a serum tryptase at least to get a baseline. If they feel they’ve had anaphylaxis or symptoms that are characteristic, potentially of an allergic reaction, I’ll try to get them to get a tryptase at that time so we can prove that mast cells as a cell of origin are bringing about this complex set of symptoms. Even that can be tricky because we’ve had a number of people with monoclonal mast cell disorders, where the aggregates on biopsy might be quite small or very limited, or with a very small amount seen on pathology. Maybe they meet some criteria, but not others have a mutation at c-KIT that’s characteristic of a mast cell disorder. If the symptoms fit, we check a tryptase. Sometimes, if I don’t really feel like the patient has a diagnosable mast cell disorder, I will go ahead and get the genetic analysis anyway and just look for the mutation. I’m sure we’re going to talk about how best to do that, but I’ll see if that would back it up, fully knowing that may not still be within the limit of detection. But that’s how we really get started. Then, I’ll frequently do an experimental treatment plan and see what the patient is responding to and if that ameliorates some of the symptoms. Thus, it’s probably a long-term thing, where you start with your assessment and you continue to assess and use whatever tools are available to try to nail down and work toward a diagnosis.
Dan DeAngelo, MD, PhD: I find these to be the most challenging patients, because the patients that I focus on are patients with systemic and mast cell activation syndrome. Of course, as you’re talking, some of these patients will just have mast cell activation syndrome, some with a clonal mast cell process, and some without. But they can be a huge challenge.
Transcript Edited for Clarity
Advertisement
Related to this article

The top 5 OncLive TV videos of the week cover insights in bladder cancer, chronic myeloid leukemia, multiple myeloma, pancreatic cancer, and chronic lymphocytic leukemia.

Two optimized CD33-directed CAR T-cell therapies generated complete remissions with incomplete count recovery in heavily pretreated relapsed/refractory AML.

Experts shared the key data that stood out in hematologic oncology at the 2026 ASCO Annual Meeting.

Ruxolitinib plus extracorporeal photopheresis drove responses in steroid-refractory or -dependent chronic graft-vs-host disease.

Readouts across LBCL, relapsed/refractory myeloma, and CALR-mutated myelofibrosis anchored the hematology data presented at EHA 2026.

In case you missed any, check out our recap of the episodes of OncLive On Air that aired in June 2026.

Hematologic oncology experts outline the top data and themes to emerge from the 2026 EHA Congress

The European Commission has approved epcoritamab plus lenalidomide and rituximab for relapsed or refractory follicular lymphoma.
Advertisement
Advertisement
Trending on OncLive
1
Frontline Sac-TMT Plus Pembrolizumab Meets PFS End Point in PD-L1–Negative, Nonsquamous NSCLC
2
The OncFive: Top Oncology Articles for the Week of 7/12
3
Five Under 5: Top Oncology Videos for the Week of 7/12
4
CD33-Directed CAR T-Cell Therapies Elicit Complete Remissions in Relapsed/Refractory AML
5