
|Videos|September 27, 2021
Chronic Myelomonocytic Cell Leukemia: Clinical Considerations
The panel of experts discuss the diagnosis and assessment of chronic myelomonocytic cell leukemia.
Advertisement
Episodes in this series

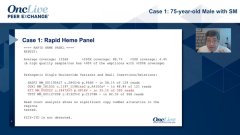





Dan DeAngelo, MD, PhD: Thank you very much. That was a great case. It reminds me of some of my cases. I think this would have been missed if you had a smaller biopsy and you might have missed that little bit of mast cell cluster. It’s important to look because I have picked up a couple of cases like this. I think it’s really driven back by the high KIT burden. The question is where does the KIT mutation occur in the hierarchy of all these other mutations? Also, if the KIT mutation is a very slow allele frequency and not representative of entire disease, then targeting that small percentage is not going to do it. But in this case, the variant allele frequency [VAF] for the KIT mutation was 41%, arguing that the clone size was greater than 80%, so the disease is probably being driven by KIT. The rest of the questions in my opinion are rather moot because SM-AHN [systemic mastocytosis with an associated hematologic neoplasm] is the disease, and then your particular example is a KIT-driven disease. Are the C findings driven from the mast portion or the CMML [chronic myelomonocytic leukemia] portion? They are all driven by KIT. Also, I would argue that this is a patient, and we have seen patients, and I have had patients, who actually respond well to KIT inhibition, either midostaurin or avapritinib. Dr Bose?
Prithviraj Bose, MD: Actually, this is a very interesting and important topic where I think every case is a little bit different. Now, what we traditionally are taught to do is to clinically assess whether the C finding is attributable to the mast cell component or to the AHN. But you bring up a very good point Dan that if the KIT VAF [variant allele frequency] is very high, then it’s a bit moot because if you can hit that target you’re going to help all the lineages that the mutation is in. The NCCN [National Comprehensive Cancer Network] guidelines also say that the clinician should first determine what is more urgent to treat and what the organ damage is stemming from. But as was shown in the avapritinib presentation at EHA [European Hematology Association annual meeting] this year, even other lineages, such as eosinophils and monocytes, can go down with avapritinib. Thus, again if KIT is the driver and it is present in more than 1 lineage, then hitting that might suffice. We don’t know that and certainly not in all cases, and I think combination therapies will be necessary, but there is some potential for a KIT-driven drug to do that.
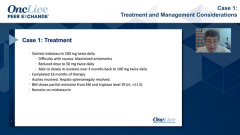
Sa Wang, MD: This was a case before avapritinib. The patient actually was treated with hypomethylating agents [HMAs], followed by allogeneic stem cell transplant, and the patient had been in remission for 3 years.
Dan DeAngelo, MD, PhD: My case was very similar, but my patient was a little bit older, not a transplant candidate, and didn’t respond to HMA therapy and then was coming in for a second referral. Actually, interestingly, she had these lesions on her skin that made me think that this patient may have SM [systemic mastocytosis]. She had classic uticaria pigmentosa. We got a tryptase level that was elevated, then went back and looked at her marrow, and sure enough she had SM-AHN. Although she didn’t respond to HMA, she responded beautifully to avapritinib, as you pointed out, and the whole clone changed. Her splenomegaly resolved, the monocytosis resolved. Thus, I think as Dr Bose has pointed out, these are difficult cases. These are complex cases, and you’re dealing with 2 different manifestations, at least pathologically. Sometimes they are somewhat distinct, but in this particular case they are really being driven by the KIT process, and this gives you another tool in the toolbox in order to treat these complex diseases.
Sa Wang, MD: The question is probably do you treat all as KIT-mutated myeloid neoplasm instead? We have also seen cases, with few patients, but no mast cell aggregates at all. Those cases I think will probably respond as well.
Dan DeAngelo, MD, PhD: As I mentioned at the beginning when I prefaced this, one of our pathologists went back and looked at all the patients who had a next-generation sequencing panel, and for those who were KIT D816V who did not have AML [acute myeloid leukemia], because you can see it in core binding factor, when we went back and looked retrospectively at the pathology, even if the pathologist had not found or did not initially detect mastocytosis, mastocytosis was seen. Thus, we had missed about 20%. These were a small subset of patients, but we had missed about 20% of cases. This is an illustrative case where there was a small mast cell component that may have been missed if you weren’t thinking, and then we went back and looked at it. We published this in the Journal of Pathology last year. Also, just to highlight the point—mutations matter and KIT D816V, if it’s not a core binding factor disease, you have to think mast cells.
Sa Wang, MD: My point is if the patient has just CMML with a KIT mutation, you look for the mast cell aggregate, you cannot find it, but this patient still probably will respond to the treatment.
Dan DeAngelo, MD, PhD:You’re right. I understand what your point is, but a lot of it is based on the tissue. If you get a bigger sample or better sample, I think mast cells are there. We were always able to go back and find it when we looked. There may be that conundrum in a patient or a sample that you’re just not able to identify it because of the tissue, but we were always able to go back and identify the mast cell component. The point is that you’ve got to think about it, and it does open the door for KIT-driven therapy.
Transcript edited for clarity.
Advertisement
Related to this article

PRAME-directed therapies represent a novel approach in the treatment of advanced melanoma.

Roswell Park Comprehensive Cancer Center investigators will deliver 21 presentations at the AHNS 12th International Conference on Head and Neck Cancer.

Pelareorep plus a checkpoint inhibitor earned FDA fast track designation for pretreated, inoperable, recurrent, or metastatic squamous cell anal carcinoma.

Older age independently predicted higher non-relapse mortality and inferior overall survival outcomes after PTCy-based unrelated donor transplant.

The IL-10–expressing anti-CD19 CAR T-cell therapy produced a 92.9% complete response rate and a 92.9% 1-year overall survival rate in high-risk relapsed/refractory DLBCL.

The top 5 OncLive TV videos of the week cover insights in bladder cancer, chronic myeloid leukemia, multiple myeloma, pancreatic cancer, and chronic lymphocytic leukemia.

The FDA approved gedatolisib in PIK3CA wild-type breast cancer, granted full approval to selpercatinib in RET fusion+ tumors, and more.

Two optimized CD33-directed CAR T-cell therapies generated complete remissions with incomplete count recovery in heavily pretreated relapsed/refractory AML.
Advertisement
Advertisement
Trending on OncLive
1
FDA Grants Fast Track Designation to Pelareorep in Pretreated SCAC
2
CD33-Directed CAR T-Cell Therapies Elicit Complete Remissions in Relapsed/Refractory AML
3
The OncFive: Top Oncology Articles for the Week of 7/12
4
Subcutaneous Pembrolizumab Faces Scrutiny Over Convenience and Cost for Patients With Cancer
5