
|Videos|September 7, 2021
Avapritinib: Approval and Clinical Practice Implications
A panel of experts share their reactions to the approval of avapritinib and discuss the clinical implications.
Advertisement
Episodes in this series






Dan DeAngelo, MD, PhD: Prithviraj, you’re a co-author with me. Your thoughts on this data and the recent approval with avapritinib [Ayvakit]? Anything you’d like to share?
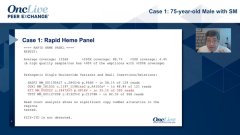
Prithviraj Bose, MD: Yes, extremely exciting, Dan. Of course, it’s been great to be a part of the avapritinib story. I think I find it very impressive that the overall response rate is 75%, not just in the PATHFINDER study, but also in the EXPLORER study, which makes it 85 evaluable patients. I think that is quite striking. Then, as you pointed out, a lot of them are CRs [complete responses]. If I recall right from the midostaurin [Rydapt] data, I think the CR rate was considerably lower…
Dan DeAngelo, MD, PhD: There were almost no true CRs. The CR plus PR [partial response] rate was about 19%, at least on the label.
Prithviraj Bose, MD: I think this is a drug which is hitting the target to a greater depth. This is, of course, a more potent and more selective inhibitor of mutant KIT, so I hope we are sparing wild-type KIT a little bit more. Not entirely, because we see myelosuppression, but hopefully more than we do with midostaurin. Overall, a very exciting drug.
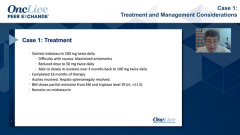
Dan DeAngelo, MD, PhD: Of course, with all due diligence, there are some toxicities of concern that are different from midostaurin. Midostaurin has the GI [gastrointestinal] intolerance, but it’s not as myelosuppressive. This agent is not horribly myelosuppressive, but it is, as you mentioned. But it does have these neurocognitive issues, and there were some cases of subdural hematomas, although those cases were predominantly in patients with thrombocytopenia. With the amendment, we only saw one. But those are issues, and management of that is going to be a thing. We have two FDA [Food and Drug Administration]-approved drugs, which is great. His is also being tested in indolent systemic mastocytosis. I’ll have a case next on that. But your thoughts Dr. Lugar?
Patricia Lugar, MD, MS: This is, quite frankly, the hope that it gives to patients and physicians alike as a real treatment, certainly a better targeted therapy, is very exciting. We have a number of patients that are very, very interested in getting enrolled in further clinical trials that have indolent. It’s just an incredibly exciting time to be managing these patients. I hope that the same symptom score for indolent as well carries over in further trials because that’s the most difficult thing—managing the chronic symptoms. Even if we know these patients are stable, they don’t have a disease that’s going to be progressive, the majority of them, but managing the day-to-day symptoms is such the burden of disease. And then, as I told you, my cocktail, not only is that exhausting and expensive, but that has a lot of side effects too—sedation, weight gain from antihistamines. It’s not easy to tolerate in seemingly very mild medications, but the burden of treatment and disease is still high on our list.
Dan DeAngelo, MD, PhD: Well, it’s always nice to have options.
Transcript edited for clarity.
Advertisement
Related to this article

The top 5 OncLive TV videos of the week cover insights in bladder cancer, chronic myeloid leukemia, multiple myeloma, pancreatic cancer, and chronic lymphocytic leukemia.

The FDA approved gedatolisib in PIK3CA wild-type breast cancer, granted full approval to selpercatinib in RET fusion+ tumors, and more.

Two optimized CD33-directed CAR T-cell therapies generated complete remissions with incomplete count recovery in heavily pretreated relapsed/refractory AML.

Lung cancer experts discuss the optimal management of CNS disease in EGFR-mutated non–small cell lung cancer.

Data for fixed-duration regimens in CLL suggest benefits over chemoimmunotherapy but still require improvements for high-risk patients.

Laure-Anne Teuwen, MD, PhD, debates the real-world advantages of subcutaneous pembrolizumab.

Iza-bren was approved in China for recurrent or metastatic ESCC following progression on platinum-based chemotherapy and PD-1/PD-L1 inhibition.

A research team from Huntsman Cancer Institute at the University of Utah showed a pathway-targeted therapy that could be an effective melanoma treatment.
Advertisement
Advertisement
Trending on OncLive
1
Frontline Sac-TMT Plus Pembrolizumab Meets PFS End Point in PD-L1–Negative, Nonsquamous NSCLC
2
The OncFive: Top Oncology Articles for the Week of 7/12
3
Five Under 5: Top Oncology Videos for the Week of 7/12
4
CD33-Directed CAR T-Cell Therapies Elicit Complete Remissions in Relapsed/Refractory AML
5